

Should we worry about body coordination in students of compulsory secondary education?
Luis Miguel Ruiz Péreza, M Gómez Garcíab, P. J. Jiménez Martínc, I Ramón Oterod, R Peñaloza Méndeze
aCatedrático. Facultad de Ciencias de la Actividad Física y Deporte (INEF). Universidad Politécnica de Madrid. España.
bProfesora de Educación Física. Centro Cultural y Educativo Reyes Católicos. Bogotá. Colombia .
cProfesor Titular. Universidad Politécnica de Madrid. España.
dBecaria FPU. Ministerio de Educación. Universidad Politécnica de Madrid. España.
eProfesor. Instituto Politécnico Nacional de México. México.
Correspondence: LM Ruiz. E-mail: luismiguel.ruiz@upm.es
Reference of this article: Ruiz Pérez LM, Gómez García M, Jiménez Martín PJ, Ramón Otero I, Peñaloza Méndez R. Should we worry about body coordination in students of compulsory secondary education? Rev Pediatr Aten Primaria. 2015;17:e109-e116.
Published in Internet: 19-06-2015 - Visits: 25046
Abstract
There is concern about the level of motor coordination among Spanish secondary students and its impact on their daily activities and health. The aim of this study was to evaluate the coordination of a sample of secondary school children. The study included 120 schoolchildren, 65 boys and 55 girls of four Secondary Schools of the Community of Madrid, aged between 12 and 14 years. All participants performed the Body Coordination Test (KKTK), designed to detect motor coordination problems in schoolchildren aged 12 to 14 years. The results allowed to establish three coordinating groups: normal (38.3%) symptomatic (31.35%) and problematic (30%). These results indicated that 61.7% of the students participating in this study formed the Symptomatic and Problematic groups. Girls were predominant in the symptomatic and problematic levels. This study confirms that motor coordination problems exist among Spanish secondary schoolchildren. This is not only an education but also a health problem because it prevents more active life styles among adolescents, especially among girls.
Keywords
● Adolescent ● Ergonomics ● Lifestyles ● Motor skill disorders ● Psychomotor developmentINTRODUCTION
It is clear that the practise of sports and physical activity in school-aged children and adolescents carries numerous benefits.1,2 Many studies have provided grounds for education and health authorities to consider increasing the number of days physical education is taught in schools, as, far from impinging on academic achievement, it contributes to it while also improving the health of students.3-5 However, the literature has shown that the interest of adolescents in these activities is progressively waning,6 while there is an alarming increase in overweight and obesity in these age groups.7
Motor coordination is considered one of the main functions of motor skills, and is the one that best predicts the likelihood of engaging in physical activity in the future.8,9 There is ample evidence that poor coordination is usually associated with low levels of physical activity,10 poor physical condition,11 unhealthy weight gain,12,13 low self-esteem,14 low self-efficacy,15 anxiety16 and even bullying.14
The estimated international prevalence of coordination problems in schoolchildren ranges between 5% and 18%. The scientific literature labels these problems as developmental coordination disorders (DCDs).17 Their prevalence in Spain has yet to be determined, and the concern among health, education and psychology professionals is low due to the dearth of studies on the subject,16 while in other regions of the world it has become the object of research and concern.9,13,18
There is a broad range of instruments mostly aimed at detecting this kind of problem, but they are rarely used by Spanish professionals. We are referring to the Motor-BOT-2 test developed by Bruininks-Oseretsky,19, the Basic Motor Ability Tests-Revised (BMAT-R),20 the McCarron Assessment of Neuromuscular Development (MAND),21 the body coordination test (KKTK)22 or the Movement Assessment Battery-2 (ABC-2), which was recently standardised and validated for the Spanish population.23
The main purpose of this study was to analyse the motor coordination level in a sample of Spanish students of compulsory secondary education by sex and age.
MATERIALS AND METHODS
Participants
One hundred and twenty students of both sexes participated on a voluntary basis, with ages ranging from 12 to 14 years (mean, 12.54 years; SD, 0.65 years), representing four public secondary schools located in urban settings of the Autonomous Community of Madrid (Spain). There were 65 male (54.2%) and 55 female students (45.8%).
Motor skills test
We used the test developed by Kiphard and Schilling to assess gross motor coordination.22 This instrument was developed to detect and diagnose coordination problems in schoolchildren aged 5 to 14 years. It assesses the dimension “gross body control and coordination” and comprises four tasks:
- Balancing while walking backwards. The student has to walk backwards one step at a time on three different balance beams, 3 m in length and of different widths (6, 4.5 and 3 cm). The number of steps the student can take on each beam is recorded.
- Hopping with one leg over an obstacle. The student is asked to jump from one leg over an obstacle made with foam blocks measuring 50 × 20 × 5 cm. The height is increased progressively for increasing age. The student has to jump at least twice more after clearing the obstacle. Both legs are assessed.
- Lateral jumping. The student has to jump laterally with both feet together from one side to the other of a slat measuring 60 × 4 × 2 cm as many times as he or she can in 15 seconds. The number of jumps performed correctly is recorded.
- Shifting platforms. The student has to move across the floor on platforms measuring 25 × 25 × 2 cm and supported by four legs that are 3.7 cm in height. Starting from one of the platforms while holding the other one, the student has to more forward without stepping off the platforms, which requires moving the platforms in the direction of the movement, stepping on one then placing the other. The number of correct relocations performed in 20 seconds is recorded.
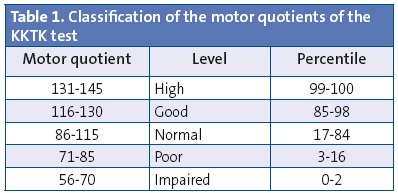
To determine the level of coordination displayed by the students, we converted the raw scores into standardised scores (motor quotient) for each of the tasks, which were later used to calculate the total motor quotient (mean, 100; standard deviation, 15) in a percentile distribution. A result of 85 or less in the total motor quotient represented motor performance below the 15th percentile. A score below 70 meant that performance was below the 3rd percentile (Table 1). The original test standards were established taking into account both age (4–5 to 14 years) and sex.
Method
We reached out to school principals and physical education teachers directly to explain the nature of the study, ask for their consent and request their collaboration. We subsequently crafted a letter explaining the study that was sent to the parents of the students to obtain their consent by signing the letter. The test was performed one student at a time in an area reserved for that purpose (classroom and/or gymnasium) during the time scheduled for physical education. The length of each individual test was of about 15 to 20 minutes.
Statistical analysis
To validate the factorial structure of the test we used factor analysis (principal component analysis) with varimax rotation. We assessed the suitability of the correlational matrix used in the analysis by means of the Kaiser-Meyer-Olkin test (KMO) and Bartlett’s test of sphericity. We tested for normality and homogeneity of variance using the Kolmogorov-Smirnov test and Levene’s test, respectively, and then carried out descriptive analyses (means and standard deviations) and comparisons by sex and age by means of multivariate analysis of variance (MANOVA). The level of statistical significance was set at 0.05 (two-sided) for all tests. We also decided to report the effect size obtained. The statistical calculations were performed with the SPSS® software version 20.0.
RESULTS
Factor analysis of the four tasks performed
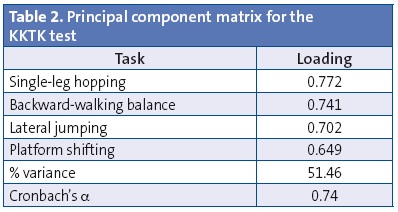
In order to confirm the unidimensionality of the test, which comprises four different tasks, we carried out a factor analysis (principal component method) with varimax rotation. Both the results of Bartlett’s test of sphericity (Χ2(6) = 72.76; P <. 000) and the measure of sampling adequacy (MSA), obtained by the overall Kaiser-Meyer-Olkin index (0.716) were satisfactory for the performance of factor analysis. The factor analysis yielded a single factor with an eigenvalue greater than 1 that explained 51.46% of the variance, loadings greater than 0.60 and a reliability of 0.74 (Table 2). These results confirmed the unifactorial structure of the test developed by its authors on the basis of a large sample of German schoolchildren.
Descriptive and comparative analyses
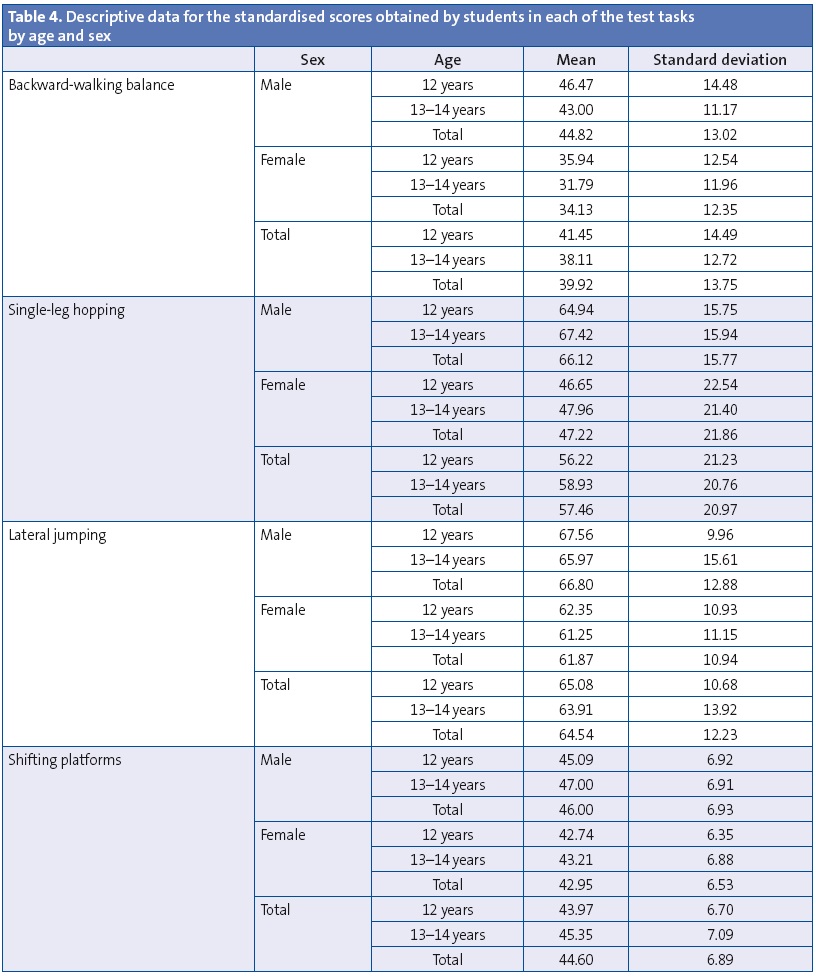
Tables 3 and 4 present the descriptive data of the scores obtained by the sample of students in each of the test tasks, both by sex and by age.

Comparative analyses
We assessed the effects of sex (male and female) and age (12 and 13–14 years) in the different tasks of the test by means of MANOVA, in which the dependent variables were the test tasks and the factors were sex and age, and we only found significant differences based on sex (Wilk’s lambda, 0.645; F, 15.57; P < .000; η2 = 0.35). Univariate analyses showed that these differences emerged in all four test tasks (backward beam walk: P = .029, η2 = 0.015; one-legged hopping: P = .000, η2=0.15; lateral jumping: P = .000, η2 = 0.026; platform shifting: P = .010, η2 = 0.05). These differences indicated that male students scored higher than their female peers.
The scores were used to classify participants into one of three groups based on their performance on the test. The mean value of the motor quotient of the male students in the sample was 88.63 (SD, 14.68) and the mean quotient for female students was 67.25 (SD, 16.60), which evinced that while the mean score of the boys fell within the range considered normal by the test standards, the mean score of the girls fell within the impairment category (see Table 1).
Forty-six schoolchildren (38.3%) were classified as having normal coordination, thirty-eight (31.7%) as having poor coordination, and thirty-six (30%) as having impaired coordination. These results show that 61.7% of schoolchildren (74 of the participants in the study) had some type of coordination problem, as their performance fell within the poor and impaired categories.
We ought to highlight that none of the students had a score exceeding 113, and thus none could be classified into the good or high coordination categories based on the reference levels. Another important finding was that girls predominated in the poor and impaired categories, especially in the 13-to-14 years age interval (Table 5), in which only one of the 24 girls had a score that fell within the range corresponding to a normal level of coordination.

DISCUSSION
The main objective of the study was to analyse the level of gross motor coordination in a sample of Spanish first-year students of ESO by means of the body coordination test.22 We found the results alarming, as 74 (61.7%) of the 120 students in the sample tested below the appropriate level (normal) of motor coordination established by the authors of the test, and were classified into the poor and impaired categories.
These results alert us to the facts already reported by previous studies, the presence in primary and secondary schools of students that have difficulty coordinating movement, a problem found in early childhood, primary, and secondary education settings. It continues to be a hidden and neglected problem among ESO students.16 The fact that none of the participants achieved a score allowing classification into the good or high categories demands that we reflect on the poor motor coordination skills of the students that participated in the study and that investigate the underlying causes of this situation.
In their 1974 study conducted on 1283 schoolchildren, the authors of the test22 found that only 2% had significant coordination problems (impaired category) and that 68% had a normal level, while 14% had good coordination and 2% a high level of motor coordination. The contrast is self-evident, as four decades later the decrease in coordination skills is quite marked in very different populations, as demonstrated by studies conducted in Portugal, Brazil, Greece, Norway, Canada, Belgium or the Netherlands.24-28
A recent study conducted in Barcelona by Torralba et al29 in Catalonian schoolchildren aged 7 to 10 years that used the same test showed similar results. In their study, which had a sample of 1254 schoolchildren, 40% exhibited some type of coordination problem, and only 4.6% was classified above the normal level. The recent study carried out by Vandorpe et al30 in Belgium reached similar conclusions, confirming a decrease in coordination skills in the four decades that have elapsed since the study on which the test was based.
In Spain, these results demand the attention of both health care and education professionals, considering that despite the fact that physical education is part of the official curriculum in schools, coordination problems still exist in the population of schoolchildren, and as we mentioned above, poor motor coordination is associated with sedentary and unhealthy lifestyles in the future.7,28,31 It is very likely that the reason why a considerable proportion of students classifies into the impaired category is a significant lack of physical activity.23,31-33 The time spent weekly in curricular physical education classes in compulsory secondary education does not exceed two hours, a clearly insufficient amount, and the percentage of students that do not do any kind of extracurricular sport or physical activity is increasingly large.
Students in the impaired category should receive especial attention and be evaluated more thoroughly, as it is likely that they meet all the necessary criteria for developmental coordination disorders (DCDs) as defined by the American Psychiatric Association.34 This is definitely a problem that concerns health care professionals as much or more than physical education teachers. If it is not addressed, these students are destined to reach adulthood with the same problems15,35 and settle into sedentary lifestyles.
Another salient finding is that most of the students in the poor and impaired categories were female. The difference in the coordination performance of male and female adolescents was considerable, especially at 13 and 14 years of age, which is consistent with the findings of the study of Catalonian students by Torralba et al.29 In our study, the female to male ratio of the 36 students (31.7%) in the impaired level was 5:1 for both age intervals. It is also worth noting that of the 46 students (38.3%) in the normal coordination level, only four of those aged 12 years and one of the 13-to-14 year olds were female. This is an alarming issue and it should be investigated in greater detail, because in light of the association between poor coordination and low levels of physical activity, girls will be more likely to develop sedentary lifestyles, with all the ensuing consequences.11
CONCLUSIONS
Several studies are bringing to our attention the deterioration of the physical condition of schoolchildren and the increasing prevalence of overweight and obesity. 36-39 Coordination skills have decreased considerably in children and adolescents, and this demands a much more proactive approach from medical and educational authorities. This study adds to the already existing body of evidence, which calls for the need to consider these problems not just in the context of education, but as a health issue in the paediatric and adolescent population.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS: DCD, developmental coordination disorders; ESO, compulsory secondary education; KMO, Kaiser-Meyer-Olkin test; MANOVA, multivariate analysis of variance; MSA, measures of sample adequacy; KKTK test, Körper Koordination Test für Kinder.
REFERENCES
- Donnelly JE, Greene JL, Gibson CA, Sullivan DK, Hansen DM, Hillman CH, et al. Physical activity and academic achievement across the curriculum (A+PAAC): rationale and design of a 3-year, cluster-randomized trial. BMC Publ Health. 2013;13:307.
- Kohl HW 3rd, Hobbs KE. Development of physical activity behaviors among children and adolescents. Pediatrics. 1998;101:549-54.
- Ahamed Y, Macdonald H, Reed K, Naylor PJ, Liu-Ambrose T, McKay H. School-based physical activity does not compromise children’s academic performance. Med Sci Sports EΧerc. 2007;39:371-6.
- Ericsson I. Motor skills, attention and academic achievements. An intervention study in school years 1-3. Brit Educ Res J. 2008;34:301-13.
- Trudeau F, Shephard RJ. Physical education, school physical activity, school sports and academic performance. Int J Behav Nutr Phys Act. 2008;5:10.
- Cocca A, Liukkonen J, Mayorga-Vega D, Viciana-Ramírez J. Health-related physical activity levels in Spanish youth and young adults. Percept Mot Skills. 2014;118:247-60.
- Arriscado Alsina D, Muros Molina JJ, Zabala Díaz M, Dalmau Torres JM. Influencia del seΧo y el tipo de escuela sobre los índices de sobrepeso y obesidad. Rev Pediatr Aten Primaria. 2014;16:e139-e146.
- Lopes VP, Rodrigues LP, Maia JA, Malina RM. Motor coordination as predictor of physical activity in childhood. Scand J Med Sci Sports. 2011;21:663-9.
- Saakslahti A, Numminen P, Niinikoski H, Rask-Nissila L. Viikari J, Tuominen J, et al. Is physical activity related to body size, fundamental motor skills, and chd risk factors in early childhood? Pediatr EΧerc Sci. 1999;11:327-40.
- Williams HG, Pfeiffer KA, O'Neill JR, Dowda M, McIver KL, Brown WH, et al. Motor skill performance and physical activity in Preschool children. Obesity (Silver Spring). 2008;16:1421-6.
- Lifshitz N, Raz-Silbiger S, Weintraub N, Steinhart S, Cermak SA, Katz N. Physical fitness and overweight in Israeli children with and without developmental coordination disorder: Gender differences. Res Dev Disabil. 2014;35:2773-80.
- Cairney J, Hay JA, Faught BE, Hawes R. Developmental coordination disorder and overweight and obesity in children aged 9-14 years. Int J Obes (Lond). 2005;29:369-72.
- Montgomery SM. Coordination, childhood weight gain and obesity. CMAJ. 2010;182:1157-8.
- Piek JP, Barrett NC, Allen LS, Jones A, Louise M. The relationship between bullying and self-worth in children with movement coordination problems. Br J Educ Psychol. 2005;75:453-63.
- Fitzpatrick DA, Watkinson EJ. The lived eΧperience of physical awkwardness: adults’ retrospective views. Adapt Phys Act Q. 2003;20:279-97.
- Gómez M, Ruiz LM, Mata E. Los problemas evolutivos de coordinación en la adolescencia: análisis de una dificultad oculta. RICYDE. Rev Int Cienc Deporte. 2006;3:44-54.
- Kadesjö B, Gillberg C. Developmental coordination disorder in Swedish 7 years-olds. J Am Acad Child Adolesc Psychiatry. 1999;38:820-8.
- Ruiz LM. Moverse con dificultad en la escuela. Introducción a los problemas evolutivos de coordinación motriz. Sevilla: Wanceulen; 2005.
- Bruininks RH. Bruininks-Oseretsky test of motor proficiency, 2nd ed (BOT™-2). EE. UU.: Pearson; 2005.
- Arnheim D, Sinclair W. El niño torpe. Un programa de terapia motriz. Buenos Aires: Médica-Panamericana; 1976.
- McCarron LT. McCarron assessment of neuromuscular development. Dallas: Common Market Press; 1982.
- Kiphard EJ, Schilling VF. Köperkoordinations-test für kinder. Beltz Test GMBH. Weinhein; 1974.
- Henderson SE, Barnett S, Sugden DA. MABC-2, batería de evaluación del movimiento para niños- 2. EE. UU.: Pearson; 2011.
- Carminato RA. Desempenho motor de escolares através da bateria de teste KTK. Dissertação de Mestrado, Universidade Federal do Paraná, Curitiba-Brasil; 2010.
- Lopes VP, Maia JAR, Silva RG, Seabra A, Morais FP. Estudo do nível de desenvolvimento da coordenação motora da população escolar (6 a 10 anos de idade) da Região Autónoma dos Açores. Rev Port Ciênc Desporto. 2003;3:47-60.
- Mjaavatn PE, Gundersen KA, Segberg V. Physical activity and health related variables in 6-9 year-old Norwegian children. Med Sci Sports EΧerc. 2003;35:S63.
- Smits-Engelsman BC, Henderson SE, Michels CGJ. The assessment of children with developmental coordination disorder in the Netherlands: The relationship between the Movement Assessment Battery for Children and the Korperkoordinations Test Fuer Kinder. Hum Mov Sci. 1998;17:699-709.
- Tsiotra GD, Nevill AM, Lane AM, Koutedakis Y. Physical fitness and developmental coordination disorder in Greek children. Pediatric EΧer Sci. 2009;21:186-95.
- Torralba MA, Vieira MB, LleiΧá T, Gorla JL. Evaluación de la coordinación motora en educación primaria de Barcelona y provincia. Rev Int Med Cienc Act Fís Deporte. 2015 [in press].
- Vandorpe B, Vandendriessche J, Lefevre J, Pion J, Vaeyens R, Matthys S, et al. The Körperkoordinations Test fur Kinder: reference values and suitability for 6–12-year-old children in Flanders. Scand J Med Sci Sports.2011;21:378-88.
- Bouffard M, Watkinson EJ, Thompson LP, Causgrove Dunn JL, Romanow SKE. A test of the activity deficit hypothesis with children with movement difficulties. Adapt Phys Act Q. 1996;13:61-73.
- Cairney J, Hay JA, Veldhuizen S, Missiuna C, Faught BE. Developmental coordination disorder, seΧ, and activity deficit over time: a longitudinal analysis of participation trajectories in children with and without coordination difficulties. Dev Med Child Neurol. 2010;52:e67-72.
- Cairney J, Hay JA, Faught BE, Corna LM, Flouris A. Developmental coordination disorder, age, and play: a test of the divergence in activity-deficit with age hypothesis. Adapt Phys Activ Q. 2006;23:261-76.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4.ª edición. Washington, DC: Author; 2006.
- Cousins M, Smyth MM. Developmental coordination impairments in adulthood. Hum Mov Sci. 2003;22:433-59.
- García Cruz A, Figueroa Suárez J, Osorio Ciro J, Rodríguez Chavarro N, Gallo Villegas J. Asociación entre el estado nutricional y las capacidades físicas en niños de 6 a 18 años de Medellín (Colombia). An Pediatr (Barc). 2014;81:343-51.
- Barnett LM, van Beurden E, Morgan PJ, Brooks LO, Beard JR. Childhood motor skill proficiency as a predictor of adolescent physical activity. J Adolesc Health. 2009;44:252-9.
- Watkinson EJ, Causgrove Dunn J, Cavaliere N, Calzonetti K, Wilhelm L, Dwyer S. Engagement in playground activities as a criterion for diagnosing developmental coordination disorders. Adapt Phys Activ Q. 2001;18:18-34.
- Casajus JA, Leiva MT, Villarroya A, Legaz A, Moreno LA. Physical performance and school physical education in overweight Spanish children. Ann Nutr Metab. 2007;51:288-96.