
Vol. 15 - Num. 58
Original Papers
Assessment of parental asthma knowledge with the Newcastle Asthma Knowledge Questionnaire
M.ª Teresa Leonardo Cabelloa, E Oceja-Setienb, L García Higueraa, M. J. Caberoa, E Pérez Belmontea, I Gómez-Aceboc
aServicio de Pediatría. Hospital Universitario Marqués de Valdecilla. Santander. España.
bGrupo de Medicina Preventiva y Salud Pública. Facultad de Medicina. Universidad de Cantabria. Santander. España.
cGrupo de Medicina Preventiva y Salud Pública. Facultad de Medicina. Universidad de Cantabria. CIBER Epidemiología y Salud Pública (CIBERESP). Instituto de Formación e Investigación Marqués de Valdecilla (IFIMAV). Santander. España.
Correspondence: MT Leonardo. E-mail: maiteleonardo@hotmail.com
Reference of this article: Leonardo Cabello MT, Oceja-Setien E, García Higuera L, Cabero MJ, Pérez Belmonte E, Gómez-Acebo I. Assessment of parental asthma knowledge with the Newcastle Asthma Knowledge Questionnaire. Rev Pediatr Aten Primaria. 2013;15:117-26.
Published in Internet: 20-06-2013 - Visits: 37563
Abstract
Objective: to determine the level of asthma knowledge in parents of asthmatic children followed in a pediatric respiratory ward.
Material and methods: descriptive and cross-sectional study. Asthma Knowledge was assessed using the Newcastle Asthma Knowledge Questionnaire (NAQK). We performed a questionnaire to parents and other relatives of asthmatic children treated in the pediatric pulmonary ward of a tertiary hospital. The surveys were conducted between September and November 2009.
Results: the sample consisted of 344 questionnaires. The mothers answered 72.7%, the fathers14.9%, both parents filled the questionnaire in 6.7% and 5.8% were filled by a different person. Patients were 203 boys (59%) and 141 girls (41%) with a mean age of 8 ± 4 years. The average score was 18.5 ± 3.7 points out of 31.
Conclusions: our respondents have obtained higher mean score compared to similar samples in other studies. Nevertheless we believe that an educational intervention can improve asthma knowledge and help decrease the morbidity of this chronic disease.
Keywords
● Asthma ● Asthma knowledge ● The Newcastle Asthma Knowledge QuestionnaireINTRODUCTION
Asthma is the most frequent chronic childhood disease in developed countries, so it has enormous repercussions not only for the individual and the family, but also at the social and economic levels1.
Its chronic character entails that there is no cure for it, and consequently the goal of treatment focuses on managing the symptoms appropriately, sustaining normal levels of physical activity and pulmonary function, and preventing exacerbations2.
In the past few years there has been an increasing emphasis on the need for healthcare professionals to devote more effort to education, an essential aspect in the treatment of any chronic disease that is also necessary in asthma2.
The increased knowledge, acquisition of the necessary skills, and improvement in the attitude and behaviours of patients, family members, and caregivers, all facilitate greater adherence to treatment and allow for the improved management of the symptoms and the disease3. This is why the current main guidelines and consensus documents for asthma management recommend educational intervention as one of the pillars of asthma management and treatment4-6.
The objective of this study is to determine the level of knowledge of asthma, and its management, of parents and family members of asthmatic children who are being monitored in our specialised care clinic, for which we used a questionnaire designed and validated for this purpose.
MATERIAL AND METHODS
Descriptive and cross-sectional study using self-report questionnaires on the knowledge of childhood asthma and its management. The questionnaire was administered to parents and family members of asthmatic children who are seen in the Childhood Pneumonology Department of the Hospital Universitario Marqués de Valdecilla (Santander, Spain). The questionnaires were administered between September and November 2009.
Asthma knowledge was evaluated using the Newcastle Asthma Knowledge Questionnaire (NAQK)7, translated and adapted to Spanish, and validated by Praena et al.8.
This questionnaire consists of 31 items and assesses the knowledge about asthma symptoms, triggers, and treatment. It has 25 true/false questions and six open-ended questions.
Right answers rate 1 point and wrong answers 0 points. The total score of the questionnaire is obtained by adding up the points for all questions. The final value ranges between 0 and 31, with a higher score indicating greater knowledge.
The open-ended questions of the questionnaire were rated by two paediatric resident doctors in their last year of training, who adhered stringently to the scoring rules for the questionnaire.
The text of the first question implies that the answer must include all of the three main symptoms of asthma, so answers have only been rated as correct when all three were enumerated.
The answer to question six has been rated as correct if the respondent named at least one of the three triggers that are established as possible answers.
Questions 10, 11, 21, and 23 have been rated as correct when the respondent has given at least two of the answers that the questionnaire offers as possible answers, as indicated by the scoring rules of the original questionnaire7,8.
The questionnaire was given to the parents or family members that accompanied the child upon arrival to the hospital, so that they could fill it in during the waiting time before the appointment. The decision to do the questionnaire was voluntary, and all the participants were given written information about our intent to carry out a study using the obtained data along with the questionnaire.
Each questionnaire also asked the respondent to write down, on a voluntary basis, his or her relationship to the child, level of studies, and whether he or she had another asthmatic child.
Other epidemiological data were gathered, such as the age of the patient, how long the patient had been monitored in the clinic (since the date of the first appointment), the diagnosis (according to the classification established in the Guía Española del Manejo de Asma, the Spanish guidelines for asthma management) and whether the patient had had any asthma-related hospitalisations.
We performed a descriptive analysis of all the variables for which data were collected. For quantitative variables we calculated the mean, the standard deviation, the median, and the interquartile range. Qualitative variables were described using the corresponding frequencies and their 95% confidence interval.
We did the statistical analysis of the data using the SPSS® software, version 20.0.
RESULTS
We gave out 500 questionnaires, of which 387 were filled in, reaching a 77.5% response rate.
We then excluded questionnaires that had been filled for patients who were not asthmatic and who had come to the clinic for another reason (cystic fibrosis, post-pneumonia follow-up, bronchiectasis, etc.), as well as questionnaires that had not been completed for whatever reason.
The final sample consisted of 344 questionnaires. The parents filled in the questionnaires, of which 72.7% were filled in by the mother of the patient, 14.9% by the father, 6.7% by both parents, and 5.8% by another person who accompanied the child (a grandmother in most cases).
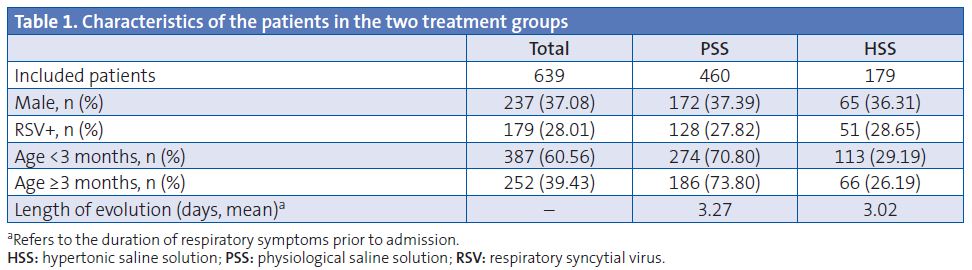
The patients were 203 boys (59%) and 141 girls (41%) with an average age of 8±4 years. Table 1 shows the main characteristics of the sample under study.
The average questionnaire score was 18.5±3.7 points.
Figure 1 shows the percentage of wrong answers and of questions left unanswered in the questionnaire.
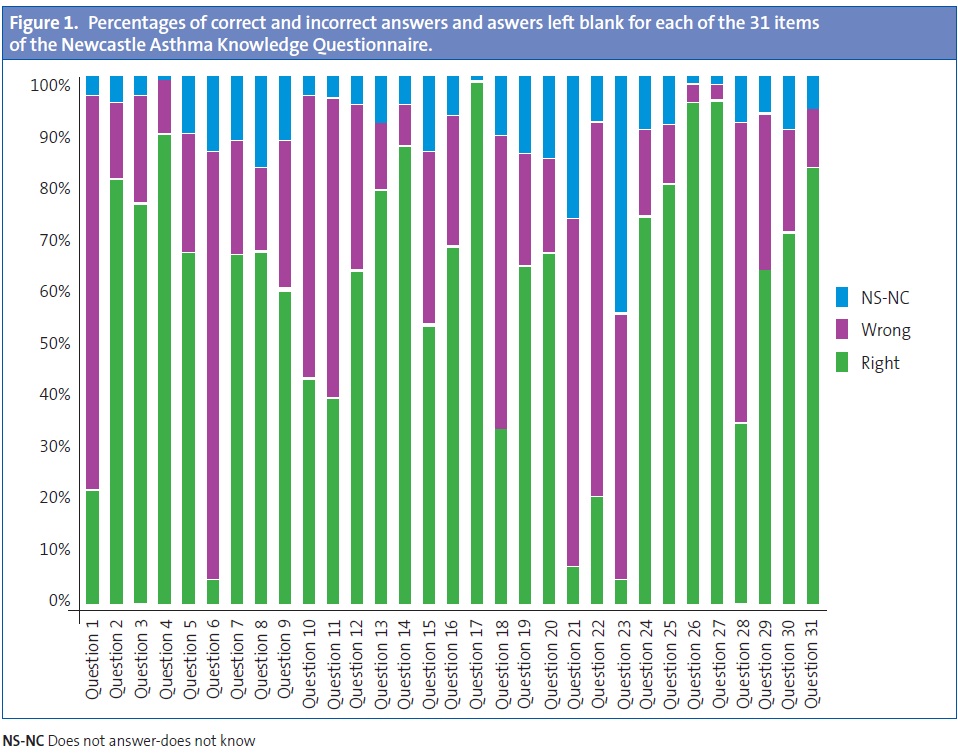
Table 2 shows the percentage of correct answers for each of the 31 items of the NAKQ. Having done a detailed analysis of the responses, we can state the following:
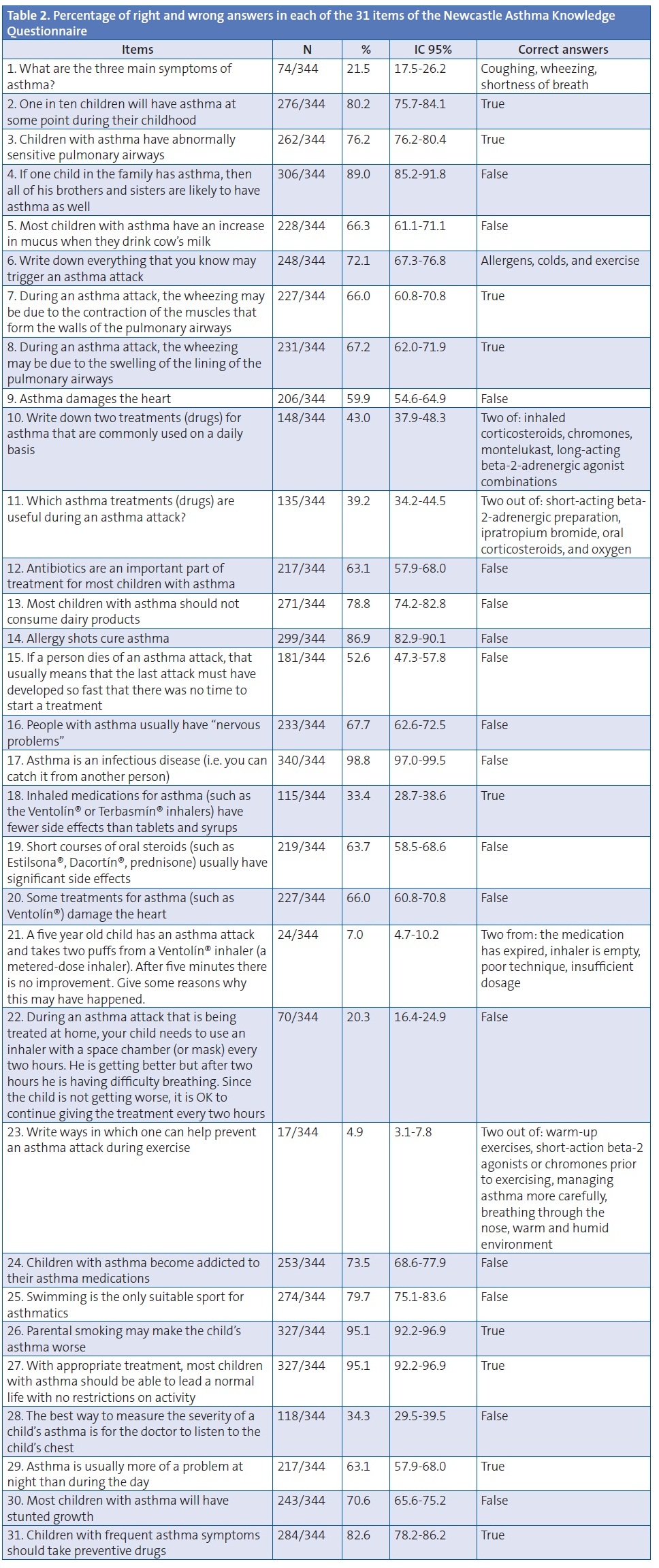
General knowledge of asthma (questions 1, 2, 3, 25, 26, 28, and 29)
When it came to general knowledge on asthma, 80.2% of the respondents knew the prevalence of childhood asthma, 76.2% knew that children with asthma have abnormally sensitive pulmonary airways, and 60% stated that asthma was not harmful to the heart.
Only 21.5% could enumerate the three main symptoms of an asthma attack. In a high percentage of cases, the parents enumerated up to two symptoms, but the scoring rules of the questionnaire specify that this answer is only considered correct if all three symptoms are enumerated (coughing, wheezing, and shortness of breath).
A very high percentage of respondents (95.1%) understood that their smoking could make their children’s asthma worse. 63% knew that asthma is usually more of a problem at night than during the day. However, 65.7% of parents believed that the best way to evaluate the severity of asthma is for a doctor to listen to the child’s chest.
Acute attack: recognition, triggers, and management (questions 6, 7, 8, 11, 15, 18, 19, 20, 21, 22, and 23)
When it came to an acute asthma attack, only 4.4% were capable of identifying the three main triggers of such an attack (colds, allergens, and exercise), but up to 29.6% of the respondents named at least two of these triggers. 66% knew that the wheezing is due to the tightening of the muscles of the pulmonary airways, or that it can also be due to the swelling of the lining of the air passages, as stated by 67.2% of the respondents.
As for the management of asthma, we ought to highlight that only 39.2% answered correctly about the medications that are used in an acute attack, and only 5% knew ways of preventing an exercise-induced asthma attack.
Only 33.4% knew that inhaled drugs have fewer side effects than oral medications, 63.7% knew that short courses of corticosteroids do not have significant side effects, and 66% stated that Ventolin® did not damage the heart.
There was a low response rate for the question that presented the challenge of an acute asthma attack that is not improving and asks for reasons why this may happen, a question that had a very low percentage of right answers (7%).
Maintenance treatment (questions 10, 12, 14, 19, 27, and 31)
When it came to asthma maintenance treatment, 63.1% knew that antibiotics are not a significant part of treatment, and 86.9% were aware that allergy shots do not cure asthma.
For the questions pertaining to medication, we considered the answer correct whether the respondent wrote the name of the active ingredient or generic name of the drug, or wrote the commercial brand name, as the respondents are not healthcare professionals. Still, the majority of parents (up to 57%) were unable to name two asthma maintenance drugs, a surprising fact considering that almost all the children who are monitored in the clinic either have been or are being treated with these medications. Furthermore, many parents believed that salbutamol is used for asthma maintenance treatment.
95% knew that with the appropriate treatment a child with asthma can lead a normal life without restrictions, and 82.6% stated that children with frequent asthma symptoms should be given preventive treatment.
False myths (questions 4, 5, 9, 13, 16, 17, 24, and 30)
When it comes to myths and beliefs about asthma, 66.3% of respondents knew that children with asthma do not experience increased mucus secretion when they drink cow’s milk, and therefore 78.8% knew that the children can consume it.
67.7% knew that asthmatic people do not usually have nervous problems, 70.6% that asthma does not cause stunted growth, and 73.5% denied that asthmatic children become addicted to their medications.
Practically all respondents (98.8%) knew that asthma is not an infectious disease.
DISCUSSION
There are several studies in Spain that have used the NAKQ questionnaire adapted and translated to Spanish by Professor Praena et al.8 to assess for knowledge of different aspects of asthma in parents and teachers9-12.
In our study we used this questionnaire, translated to Spanish, in parents of asthmatic children. The average score was 18.5 points, higher than the average score achieved by teachers (17.9 points), asthmatic adolescents (17.24 points) and adolescents without asthma (16.23 points) in the asthma study carried out in schools by Praena9, and also higher than the average score obtained by the teachers of the Estudio sobre el Asma en los Centros Escolares Españoles (Asthma Study in Spanish Schools, or EACEE, 16 points)11.
Some studies in other countries that have used the same questionnaire for asthmatic adolescents12 and for teachers13 also reported lower scores.
In the original study done in 1990 by Fitzclarence and Henry7 to validate the questionnaire, two groups of respondents were recruited, one “high knowledge” and one “low knowledge”, whose mean scores in the questionnaire were of 25 and 13 points, respectively.
In contrast to this, in the study that was done to validate the translation to Spanish of this questionnaire8 on a population of parents with high knowledge of the disease (parents of children with asthma that had benefited from an educational intervention) versus parents with low knowledge of it (who had no association to the disease or its treatments), the scores they obtained were of 23 and 16.8, respectively. Thus, the results obtained by the parents in our study are placed in between those obtained by the parents with high and low levels of knowledge in the Praena8 and Fitzclarence7 studies.
A study done in Malaysia in 2002 shows the scores of the NAKQ questionnaire in parents of asthmatic children who were admitted to the hospital for an exacerbation14. This parent sample obtained a lower score (15.5 points) than the parents in our study. The parents in Henry’s study15 also achieved lower scores.
In the recent study of García Luzardo16 done with parents of asthmatic children who had sought emergency room services for an acute attack, the average score for the NAKQ was 16.14, which is low in comparison to our results.
Thus, compared to other studies done with parents of asthmatic children, our sample of parents is more knowledgeable, as reflected by their higher questionnaire scores. Still, it is somewhat surprising that even though they are the parents of a group of patients that are being monitored in a specialised hospital clinic, which would allow the assumption that their children’s disease has had a longer course or has greater severity, their knowledge of some aspects of asthma is low and could certainly improve.
When it came to question 10, 43% identified correctly two drugs that are used for the preventive treatment of asthma, a figure that was higher than that obtained in the EACEE11, which was 3%, in the Korta study10, with 2.6% of the teachers answering correctly, and higher than the one averaged by the students and teachers in Praena’s study9. To a certain extent, it makes sense that the parents in our study achieved a higher score than the teachers in the other studies we have mentioned, as in the majority of cases these medications are administered at home and at hours when the children are not in school.
The same happened when it came to the treatment that needed to be given during an asthma attack. In our study, this was known by 39.2% of the surveyed parents, a figure that was once again higher than the 8.6% of the EACEE, the 11% of the Korta study, and the 7.9% of the teachers in the 2012 Praena study.
We think that it is of interest that we contribute to the literature the results obtained with this asthma knowledge questionnaire in a large sample of parents of asthmatic children, since in Spain the NAKQ has been used mostly to assess the knowledge in education professionals9-11. Thus, we are providing data that can be used for comparisons with other samples of parents under similar conditions.
About the questionnaire: its strong and weak points
The use of validated questionnaires is important because it allows for the comparison of different studies17.
There are several questionnaires that were developed to analyse asthma knowledge17-19. The NAKQ has been proven to be a valid instrument to evaluate asthma knowledge in parents and caregivers of asthmatic patients7,8.
Access to the NAKQ questionnaire was easy and affordable, as it can be found on the web and its distribution is free.
We faced some difficulties with the interpretation of some questions, and in our opinion their answers did not reflect a greater or lesser knowledge by the respondents; they are questions 15 and 22.
We must take into account that culture has an effect as an independent factor in the number of correct answers, as was demonstrated in the validation studies for the questionnaire, for both the English7 and the Spanish8 versions.
Furthermore, in the original paper there were up to five questions (4, 7, 17, 26, and 27) that did not show any statistically significant differences between high and low asthma knowledge groups when the answers were analysed. The same thing happened in the Spanish questionnaire validation study, where the number of items for which they found no significant differences rose to ten (questions 2, 3, 4, 7, 17, 22, 26, 28, 29, and 30). As recommended by the authors of both of these papers, the questionnaire ought to be revised in order to improve it and eliminate non-discriminating items.
We should note that in our study as well as in every other published study that has used this questionnaire9-13, the open-ended questions (1, 6, 10, 11, 21, and 23), which referred to the main symptoms of asthma, the medication to be administered, and how to proceed when there is an attack or prior to physical activity, were the questions with the lowest rates of correct answers (Fig. 1). This may be due to the greater difficulty posed a priori by an open-ended question in comparison to a dichotomous answer or even a multiple-choice answer, as demonstrated in the study done by Bruzzesse20, in which the parents were capable of identifying a larger number of triggers for asthma attacks when they were given various options from which to choose as opposed to being presented with an open-ended question.
In our study, only 21.5% were able to identify the three main symptoms of asthma, a percentage considerably higher than the 8.6% obtained by the teachers of the EACEE and the 3.4% obtained by the teachers in the Korta study10 prior to an educational intervention, and was very similar (20.8%) to that of the teachers in the study by Praena9 and to the results published in Gibson’s paper12 (21.7%).
Still, our figure is below the 45.3% achieved by parents in the Bell study18, which may be due to a difference in the scoring rules.
Our main conclusion after analysing the results was that, although compared to most of the studies done under similar conditions our respondents have a higher level of asthma knowledge–reflected by a higher mean score–we should make a point of investing more in educational intervention efforts with the asthma patient and the caregivers, as such interventions would probably lead to better control of the disease, fewer relapses, fewer hospital admissions, and ultimately to an improved quality of life for these patients.
ACKNOWLEDGMENTS
We want to thank the cooperation of the parents of the children that are seen in our clinic who filled in the questionnaires, as well as all the other staff that helped by giving out and collecting these surveys.
We also want to thank Dr. Praena et al. for their generosity in allowing us to use this questionnaire.
CONFLICT OF INTERESTS
The authors declare that they had no conflict of interests when it came to preparing and publishing this paper.
ACRONYMS: EACEE: Asthma Study in Spanish Schools • NAKQ: Newcastle Asthma Knowledge Questionnaire.
BIBLIOGRAPHY
- Masoli M, Fabian D, Holt S, Beasley R. Global burden of asthma. Developed for the global initiative for asthma. Medical Research Institute of New Zealand. Wellington, New Zealand 2006 [on line] [updated on 2011 November; consulted on 19/04/2013]. Available at www.ginasthma.org/local/uploads/files/GINABurdenReport_1.pdf
- Korta Murua J, López-Silvarrey Varela A. Asma, educadores y escuela. An Pediatr (Barc). 2011;74(3):141-4.
- Korta Murua J, Valverde Molina P, Praena Crespo M, Figuerola Mulet J, Rodríguez Fernández-Oliva CR, Rueda Esteban S, et al. La educación terapéutica en el asma. An Pediatr (Barc). 2007;66:496-551.
- National Hearth Lung and Blood Institute, National Asthma Education and Prevention Program. Expert Report 3 (NAEP EPR-3). Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institute of Health, 2007 [on line] [consulted on 19/04/2013]. Available at www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. Updated 2009 [on line] [consulted on 19/04/2013]. Available at www.ginasthma.org
- Castillo Laita LA, de Benito Fernández FJ, Escribano Montaner A, Fernández Benítez P, García de la Rubia S, Garde Garde, et al. Consenso sobre el tratamiento del asma en pediatría. An Pediatr (Barc). 2007;67:257-73.
- Fitzclarence CA, Henry RL. Validation of an asthma knowledge questionnaire. J Paediatr Child Health. 1990;26:200-4.
- Praena Crespo M, Lora Espinosa L, Aquino Linares N, Sánchez Sánchez A, Jiménez Cortés A. Versión española del NAKQ. Adaptación transcultural y análisis de fiabilidad y validez. An Pediatr (Barc). 2009;70:209-17.
- Praena Crespo M, Fernández Truan JC, Aquino Llinares N, Murillo Fuentes A, Sánchez Sánchez A, Gálvez González J, et al. Situación de los conocimientos, las actitudes y la calidad de vida en asma de adolescentes y profesorado. Necesidad de educar en los centros de enseñanza. An Pediatr (Barc). 2012;77(4):236-46.
- Korta Murua J. Impacto de una intervención educativa sobre asma en los profesores. An Pediatr (Barc). 2012;77(4):226-35.
- López-Silvarrey Varela A. Estudio sobre el asma en los centros escolares españoles (EACEE) 2009-2010. A Coruña: Fundación María José Jove; 2011 [on line] [consulted on 19/04/2013]. Available at www.fundacionmariajosejove.org/media/upload/files/Maqueta_final_publicacin_resultados_Estudio_Asma_Nacional_FMJJ_FBBVA_en_11.pdf
- Gibson PG, Henry RL, Vimpani GV, Halliday J. Asthma knowledge, attitudes, and quality of life in adolescents. Arch Dis Child. 1995;73:321-6.
- Henry RL, Gibson PG, Vimpani GV, Francis JL, Hazell J. Randomized controlled trial of a teacher-led asthma education program. Pediatr Pulmonol. 2004;38:434-42.
- Fadzil A, Norzila MZ. Parental Asthma Knowledge. Med J Malaysia. 2002;57:474-81.
- Henry RL, Cooper DM, Halliday JA. Parental asthma knowledge: its association with readmission of children to hospital. J Paediatr Child Health. 1995;31:95-8.
- García-Luzardo MR, Aguilar-Fernández AJ, Rodríguez-Calcines N, Pavlovic-Nesic S. Conocimientos acerca del asma de los padres de niños asmáticos que acuden a un servicio de urgencias. Acta Pediatr Esp. 2012;70(5):196-203.
- Rodríguez Martínez C, Sossab MP. Validación de un cuestionario de conocimientos acerca del asma entre padres o tutores de niños asmáticos. Arch Bronconeumol. 2005;41:419-24.
- Bell HM, Mcelnay JC, Hughes CM, Gleadhill I. Primary schoolteachers' knowledge of asthma: the impact of pharmacist intervention. J Asthma. 2000;37:545-55.
- Clark NM, Mitchell HE, Rand CS. Effectiveness of educational and behavioral asthma interventions. Pediatrics. 2009;123(suppl 3):S185-S192.
- Bruzzese JM, Unikel LH, Evans D, Bornstein I, Surrence K, Mellins RB. Asthma knowledge and asthma management behaviour in urbanelementary school teachers. J Asthma. 2010;47:185-91.