


Incidence of type I diabetes mellitus in the department of Elda (Alicante, Spain)
Eva González Olivaa, M.ª de los Ángeles Cuenca Alcaraza, Fernando Antonio Aleixandre Blanquera
aServicio de Pediatría. Hospital General Universitario de Elda. Elda. Alicante. España.
Correspondence: E González . E-mail: evagonzlezoliva@gmail.com
Reference of this article: González Oliva E, Cuenca Alcaraz MA, Aleixandre Blanquer FA. Incidence of type I diabetes mellitus in the department of Elda (Alicante, Spain). Rev Pediatr Aten Primaria. 2022;24;e87-e91.
Published in Internet: 12-04-2022 - Visits: 4266
Abstract
Introduction: it is essential to have studies on the prevalence of type 1 diabetes mellitus by country and region in order to be able to know the impact of the disease, the characteristics of the children and the calculation of care needs.
Material and methods: prospective study of children diagnosed between years 2011 and 2019 in the health district of Elda (Alicante, Spain). Patients were aged 0 to 14 years. We compared the results with a previous series, carried out with the same methodology in the 1988-1992 period.
Results: the incidence of diabetes mellitus in years 2011-2019 was 21.02 per 100 000 inhabitants per year. We did not detect an increase compared to the previous period. The median age at onset was 8 years. In children under 5 years, the incidence was 13.97 per 100 000 inhabitants per year. The frequency of ketoacidosis at onset decreased from 77% to 25.4%. Only 5 children were not Spanish nationals. The mode of the length of stay was 8 days.
Conclusions: the incidence of diabetes mellitus did not increase in the two periods under study. The frequency of ketoacidosis as the presentation at onset has decreased substantially. The mode of the age at diagnosis was 8 years. Children under 5 years had the lowest incidence but presented more frequently with ketoacidosis.
Keywords
● Diabetes mellitus type 1 ● Epidemiology ● IncidenceINTRODUCTION
In 1983, a group of experts meeting in Philadelphia (USA) highlighted the importance of having frequent and regularly updated statistics and healthcare records to ascertain the incidence of diabetes mellitus.1 In 1994 we first reported an incidence of type 1 diabetes mellitus (T1DM) of 16.7 per 100 000 population per year in children aged from 0 to 14 years in a health district in the Valencian Community (VC) (Elda, Alicante, Spain).2 Since then, other authors have studied the incidence of this disease in Spain1-8 and a doctoral thesis has been produced covering all the health districts in the VC.4 After this first contribution we continued collecting incidence data, since the vast majority of new diabetes cases in children in our health district receive attention at the only hospital owned and managed by the public healthcare system, and more particularly since 2019, when the Valencian healthcare system started offering all patients under the age of 14 continuous interstitial glucose monitors free of charge.
MATERIAL AND METHODS
The primary data source was the records of hospital admissions and of the service itself. As a secondary source of information we obtained the list of all patients with the following ICD-9 diagnoses: 250.01, 250.0, 250,250.1, 250.11, 250.13, 250.03, 250.21, 250.23, 250.31, through the ABUCASIS program, widely used in primary care centres and hospitals. All of them were diagnosed before the age of 15 years. Using this method we identified 55 patients in the primary source and 42 in the secondary source. We obtained the population data from the official reports of Elda health district, which downloads them, in turn, from the National Statistics Institute (INE). We used the Chapman formula3 to calculate the exhaustiveness of the primary records. We made use of previous data from our health district to make comparisons, since the methodology employed was the same. The form of presentation at diagnosis was classified as 1) diabetic ketoacidosis (DKA) if pH < 7.2 and bicarbonate < 15 mEq/l, 2) hyperglycaemia with ketonuria, and 3) hyperglycaemia without ketonuria. We calculated the annual and global incidence and the 95% confidence interval (95% CI) assuming that the new cases follow a Poisson distribution. For the continuous variables we express the results as mean, standard deviation, median and mode; for the categorical variables we present percentages. To compare means we used the Student t test. Linear correlations were performed between the continuous quantitative variables. We used p <0.05 for significance.
RESULTS
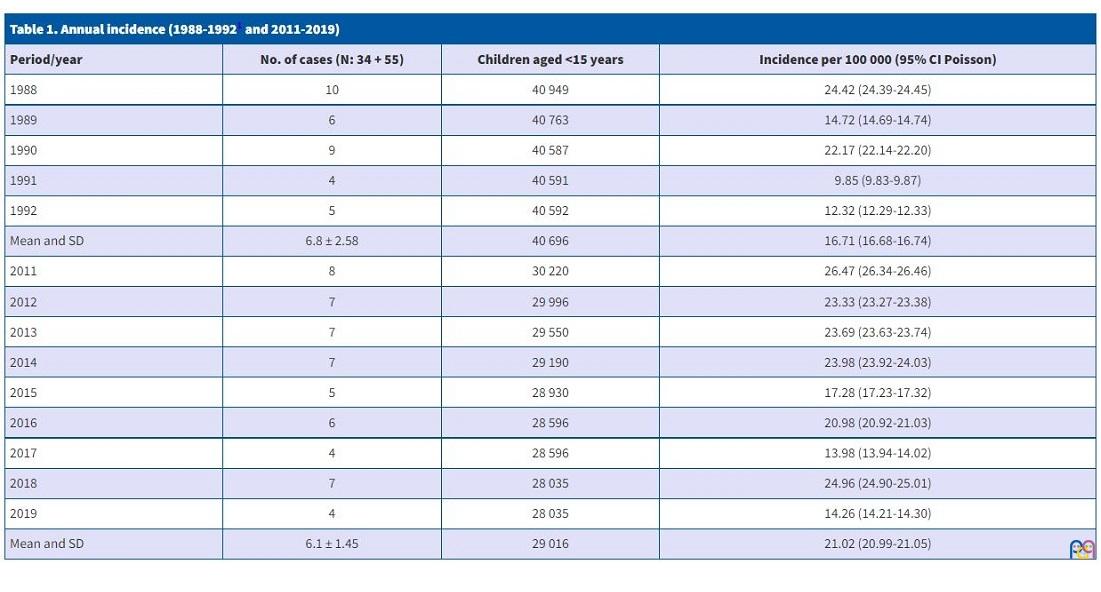
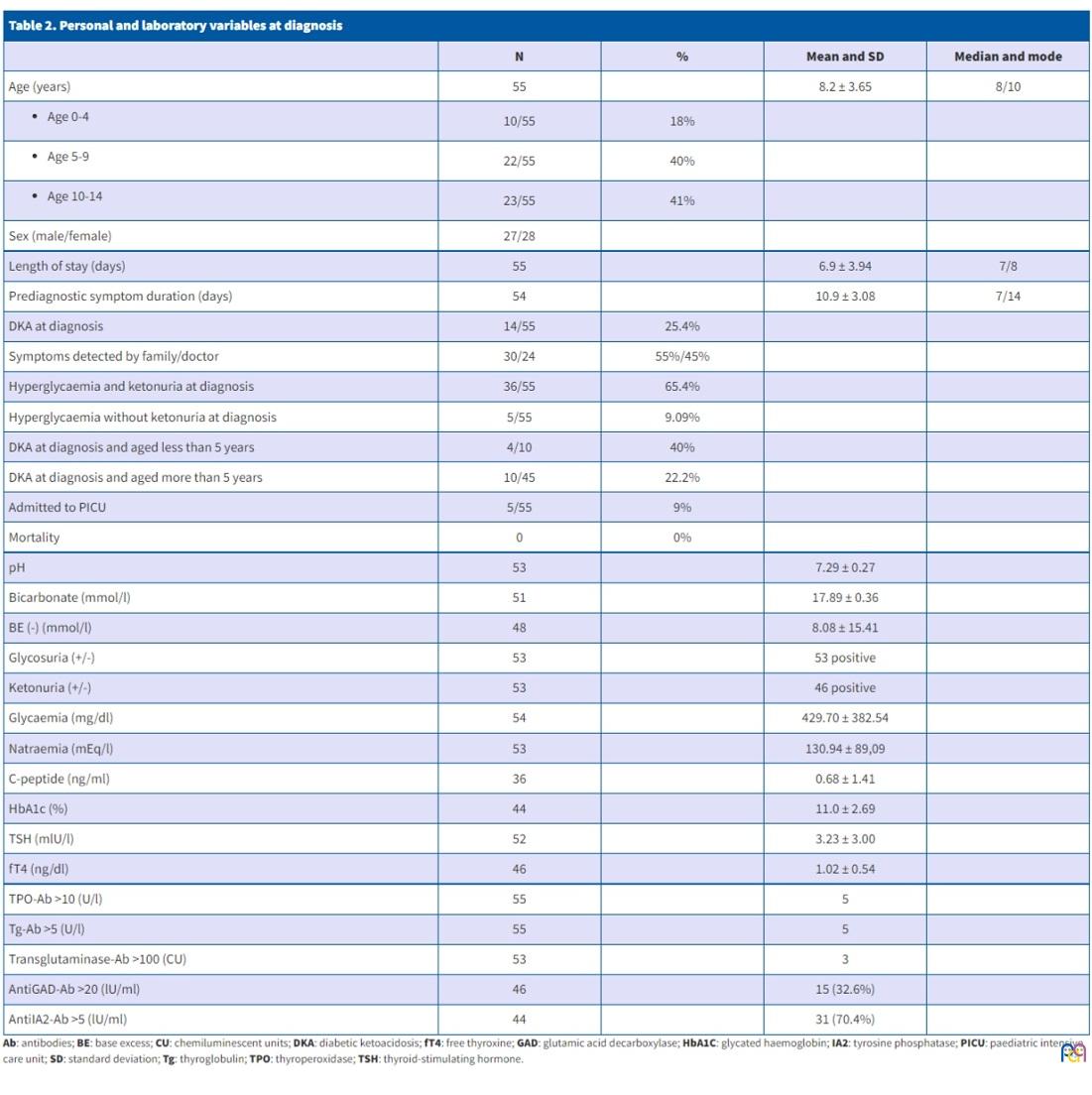
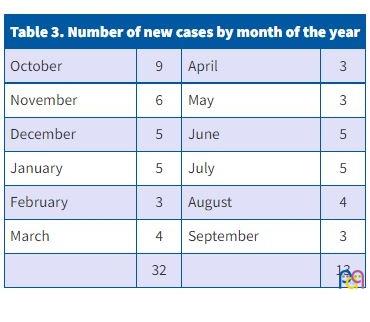
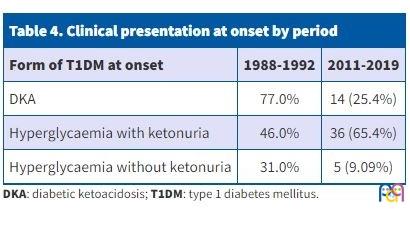
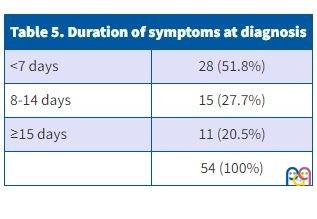
According to the Chapman formula, the confidence level of the first source was 96.4% and that of the records was 96.4%. The incidence for the years studied (2011-2019) was 21.02 (95% CI: 20.99-21.05) per 100 000 children aged 0-14 per year. There was no significant difference between the two study periods (1988-1992 and 2011-2019) (Table 1). There was no difference by sex: 27 (49%) boys and 28 (51%) girls. Place of birth was 52 (94.5%) in Spain and 3 (5.5%) in other countries (Switzerland, Paraguay, Venezuela). Mean age was 8.25 ± 1.41 years. Five children (3.6%) were aged less than 2 years and 10 (18%) less than 5 years (the incidence for those under 5 was 13.97 per 100 000 children per year). The onset was noticed by the family in 30 cases (54.5%) and by the paediatrician in 25 (45.4%). Table 2 presents the social, clinical and laboratory characteristics of the patients at diagnosis. New cases clustered significantly in the colder months (October-March) with 32 cases (p <0.001) (Table 3). Table 4 summarises the clinical presentations at onset in the two periods, and Table 5 the days elapsed between onset and diagnosis. We detected significant correlations between the following variables: pH-bicarbonate (r = 0.6; p <0.0001); pH-base excess (BE) (r = 0.657; p <0.0001); pH-glycaemia (r = −0.292; p <0.038); glycaemia-natraemia (r = −0.296; p <0.033).
| Table 1. Annual incidence (1988-19921 and 2011-2019) | |||
|---|---|---|---|
| Period/year | No. of cases (N: 34 + 55) | Children aged <15 years | Incidence per 100 000 (95% CI Poisson) |
| 1988 | 10 | 40 949 | 24.42 (24.39-24.45) |
| 1989 | 6 | 40 763 | 14.72 (14.69-14.74) |
| 1990 | 9 | 40 587 | 22.17 (22.14-22.20) |
| 1991 | 4 | 40 591 | 9.85 (9.83-9.87) |
| 1992 | 5 | 40 592 | 12.32 (12.29-12.33) |
| Mean and SD | 6.8 ± 2.58 | 40 696 | 16.71 (16.68-16.74) |
| 2011 | 8 | 30 220 | 26.47 (26.34-26.46) |
| 2012 | 7 | 29 996 | 23.33 (23.27-23.38) |
| 2013 | 7 | 29 550 | 23.69 (23.63-23.74) |
| 2014 | 7 | 29 190 | 23.98 (23.92-24.03) |
| 2015 | 5 | 28 930 | 17.28 (17.23-17.32) |
| 2016 | 6 | 28 596 | 20.98 (20.92-21.03) |
| 2017 | 4 | 28 596 | 13.98 (13.94-14.02) |
| 2018 | 7 | 28 035 | 24.96 (24.90-25.01) |
| 2019 | 4 | 28 035 | 14.26 (14.21-14.30) |
| Mean and SD | 6.1 ± 1.45 | 29 016 | 21.02 (20.99-21.05) |
| Table 2. Personal and laboratory variables at diagnosis | ||||
|---|---|---|---|---|
| N | % | Mean and SD | Median and mode | |
| Age (years) | 55 | 8.2 ± 3.65 | 8/10 | |
|
10/55 | 18% | ||
|
22/55 | 40% | ||
|
23/55 | 41% | ||
| Sex (male/female) | 27/28 | |||
| Length of stay (days) | 55 | 6.9 ± 3.94 | 7/8 | |
| Prediagnostic symptom duration (days) | 54 | 10.9 ± 3.08 | 7/14 | |
| DKA at diagnosis | 14/55 | 25.4% | ||
| Symptoms detected by family/doctor | 30/24 | 55%/45% | ||
| Hyperglycaemia and ketonuria at diagnosis | 36/55 | 65.4% | ||
| Hyperglycaemia without ketonuria at diagnosis | 5/55 | 9.09% | ||
| DKA at diagnosis and aged less than 5 years | 4/10 | 40% | ||
| DKA at diagnosis and aged more than 5 years | 10/45 | 22.2% | ||
| Admitted to PICU | 5/55 | 9% | ||
| Mortality | 0 | 0% | ||
| pH | 53 | 7.29 ± 0.27 | ||
| Bicarbonate (mmol/l) | 51 | 17.89 ± 0.36 | ||
| BE (-) (mmol/l) | 48 | 8.08 ± 15.41 | ||
| Glycosuria (+/-) | 53 | 53 positive | ||
| Ketonuria (+/-) | 53 | 46 positive | ||
| Glycaemia (mg/dl) | 54 | 429.70 ± 382.54 | ||
| Natraemia (mEq/l) | 53 | 130.94 ± 89,09 | ||
| C-peptide (ng/ml) | 36 | 0.68 ± 1.41 | ||
| HbA1c (%) | 44 | 11.0 ± 2.69 | ||
| TSH (mlU/l) | 52 | 3.23 ± 3.00 | ||
| fT4 (ng/dl) | 46 | 1.02 ± 0.54 | ||
| TPO-Ab >10 (U/l) | 55 | 5 | ||
| Tg-Ab >5 (U/l) | 55 | 5 | ||
| Transglutaminase-Ab >100 (CU) | 53 | 3 | ||
| AntiGAD-Ab >20 (lU/ml) | 46 | 15 (32.6%) | ||
| AntiIA2-Ab >5 (lU/ml) | 44 | 31 (70.4%) | ||
| Table 3. Number of new cases by month of the year | |||
|---|---|---|---|
| October | 9 | April | 3 |
| November | 6 | May | 3 |
| December | 5 | June | 5 |
| January | 5 | July | 5 |
| February | 3 | August | 4 |
| March | 4 | September | 3 |
| 32 | 13 | ||
| Table 4. Clinical presentation at onset by period | ||
|---|---|---|
| Form of T1DM at onset | 1988-1992 | 2011-2019 |
| DKA | 77.0% | 14 (25.4%) |
| Hyperglycaemia with ketonuria | 46.0% | 36 (65.4%) |
| Hyperglycaemia without ketonuria | 31.0% | 5 (9.09%) |
| Table 5. Duration of symptoms at diagnosis | |
|---|---|
| <7 days | 28 (51.8%) |
| 8-14 days | 15 (27.7%) |
| ≥15 days | 11 (20.5%) |
| 54 (100%) | |
DISCUSSION
After studying two different periods of time we did not find a significant increase in the incidence of T1DM in our health district in these years; however, other Spanish authors have perceived increases of up to 42% in their series, especially in the last 5 to 10 years.3,4 In both periods, our incidence figures, like those of the VC as a whole, show high to very high values according to WHO standards (>20 per 100 000).4 We have two extensive reviews, one in the VC and the other national, with mean incidence figures of 19.1 per 100 0004 and 17.69 per 100 0001 respectively, and with variations in Spain from 11.5 in Asturias to 27.6 in Castilla-La Mancha.1 The lowest figures in Spain were for the Balearic Islands, with 7.9 per 100 000, and the highest in Murcia, with 30.14 per 100 000.4
With respect to sex and mean age at diagnosis, the figures for our two series were similar to each other and to those of the VC as a whole4 and in line with national and international data, which show that 45% of children throughout the world are diagnosed below the age of ten years.10 The same is true of the mode.3,4 Those under the age of 5, in our two series and in studies by other authors, are the least represented age group, and although the Spanish study did not provide a breakdown by age group, there is nothing to suggest that it differed in this aspect.4,7,8 A noteworthy case is Cantabria, which has reported an increase of 35% in this age group between 2010 and 2019.5
Where we did observe a significant change was in the clinical form at diagnosis. Whereas in our first series the percentage of ketoacidosis was unacceptably high, in this second series the figures are more in line with most other studies, showing a reduction of more than 60%. Conversely, hyperglycaemia increased as a form of onset.2,9
Most series give ketoacidosis figures of 25%-40%, and even higher in those up to 4 years of age.4 An extensive multicentre study found a 39.5% rate of DKA at diagnosis, rising to 51.7% in the 0-4 year age group.1 In our series, diabetes in children under 5 began as DKA 1.8 times more frequently than in those above that age. It is also interesting to highlight the fact that in our series and in the VC, children are diagnosed with T1DM earlier (79.5% and 40.4%, respectively, diagnosed less than two weeks after onset) compared to other autonomous communities and the EURODIAB study (25%).4
In approximately half our patients, diabetes was suspected by the family, suggesting that the population has a good level of knowledge of the disease, fostered by the high prevalence of all types of diabetes. In the series for the whole of the VC, the diseases most commonly found in the family medical history were T2DM and T1DM.4
We found a very small number of children born outside Spain or resident for less than a year before diagnosis, whereas in the study of the VC as a whole the proportion was 17.4%, with a significant upward trend in the last few years.4 There were other special circumstances in families with at least one foreign parent: it was less often the families that suspected or detected diabetes, and ketoacidosis was present at diagnosis more frequently than in Spanish families. Social and work-related factors (vulnerability, working hours, language barriers, and so on) certainly lie at the root of these differences.4
Both on this occasion and in the previous study, we found a concentration of new cases in the colder months, as other authors have.2,3,4,7,12
With regard to the analytical results, the figures for HbA1c and C-peptide are no different from those for the VC as a whole; the former do prove to be higher and the latter lower in the group with ketoacidosis at diagnosis.4 The anti-pancreatic antibodies we found most frequently were anti-GAD and anti-IA2, whereas in the VC it was anti-IA2 and anti-ICA.4 Five patients had autoimmune thyroiditis, which can reach more than 40% in some countries.6
We would not like to finish without pointing out that the mode of the length of stay after diagnosis was 8 days, with a median of 7 days. This seems too prolonged a stay to us, although it can be explained by the lack of a nurse with specific training in diabetes education in this department since it first opened in 1983.11
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare. This study has received no funding.
ABBREVIATIONS
DKA: diabetic ketoacidosis · VC: Valencian Community · T1DM: type 1 diabetes mellitus · T2DM: type 2 diabetes mellitus · 95% CI: 95% confidence interval.
REFERENCES
- Conde Barreiro S, Rodríguez Rigual M, Bueno Lozano G et al. Epidemiología de la diabetes mellitus tipo 1 en menores de 15 años en España. An Pediatr (Barc). 2014;81:189.e1-e12.
- Aleixandre FA. Incidencia de la diabetes mellitus tipo I en población infantil de 0 a 14 años (1988-1992). Act Pediatr Esp. 1994;52:147-52.
- López Siguero JP, Martínez-Aedo Ollero MJ, Moreno Molina JA, Lora Espinosa A, Martínez Valverde A. Evolución de la incidencia de la diabetes mellitus tipo I en niños de 0 a 14 años en Málaga (1982-1993). An Esp Pediatr. 1997;47:17-22.
- Del Castillo C. Estudio epidemiológico de diabetes mellitus tipo 1 en población pediátrica de la Comunidad Valenciana. Universitat de València. 2020. [Accessed 03/03/2022]. Available at: https://roderic.uv.es/bitstream/handle/10550/75356/TESIS%20FINAL%20pdf%20FEBRERO%202020%20defensa%20JULIO%202020.pdf?sequence=1
- García Ibáñez Y, Freijo Martín MC. Estudio de la diabetes tipo 1 en la edad pediátrica durante la última década. Rev Pediatr Aten Primaria (Suppl). 2020;29:10-1.
- Valdés Alonso MC, Basain Valdés JM, Llópiz Herrera l, de la Rosa A, Álvarez Álvarez A. Enfermedades tiroideas en adolescentes con diabetes mellitus tipo 1. Rev Pediatr Aten Primaria. 2017;19:249-57.
- Conde Bareriro S, Rodriguez Rigual M, Bueno Lozano G. Registro de diabetes mellitus tipo 1 en Aragón: 20 años de seguimiento. Rev Esp Endocrinol Pediatr. 2013;4:13-21.
- Escribano Muñoz A, Martos Tello JM, Valcárcel Díaz I, Gutierrez Macías A. Revisión del debut de diabetes tipo 1 en hospital terciario: 2003-2007. An Pediatr (Barc). 2008;68:98-152.
- Galán l, Ortiz l, Aleixandre FA, Jover J. Reducción de la frecuencia de la cetoacidosis diabética en niños de 0-14 años. Acta Pediatr Esp. 2007;65:309.
- Dabelea D, Bell RA, D’Agostino RB, Imperatore G, Johansen JM, Linder B, et al. Incidence of Diabetes in Youth in the United States. JAMA. 2007;297:2716.
- Hospital General de Elda, Alicante. https://es.wikipedia.org/wiki/Hospital_General_de_Elda
- López Siguero JP, Lora Espinosa A, Martínez MJ. Incidencia de IDDM en niños (0-14 años) en Málaga, 1982-1988. An Esp Pediatr. 1992;37:485-8.
Comments
This article has no comments yet.