

Vol. 23 - Num. 92
Original Papers
Nationwide multicentre study on the organization of primary care paediatrics services in the first wave of the COVID-19
Beatriz Morillo Gutiérreza, M.ª Rosa Albañil Ballesterosb, Mamiko Onodac, Rafael Jiménez Alésd, M.ª Pilar Lupiani Castellanose, Josefa Ares Álvarezf, Yolanda Martín Peinadorg, Grupo de Patología Infecciosa (GPI)h
aPediatra. CS Aracena. Huelva. España.
bPediatra. CS Cuzco. Fuenlabrada. Madrid. España.
cPediatra. CS Valdelasfuentes. Alcobendas. Madrid. España.
dPediatra. Consultorio La Roda de Andalucía. Sevilla. España.
ePediatra. CS Joaquín Pece. San Fernando. Cádiz. España.
fPediatra. CS Virgen Peregrina. Pontevedra. España .
gPediatra. CS Goya. Madrid. España.
hAsociación Española de Pediatría de Atención Primaria (AEPap).
Correspondence: B Morillo. E-mail: beatriz.morillo.sspa@juntadeandalucia.es
Reference of this article: Morillo Gutiérrez B, Albañil Ballesteros MR, Onoda M, Jiménez Alés R, Lupiani Castellanos MP, Ares Álvarez J, et al. Nationwide multicentre study on the organization of primary care paediatrics services in the first wave of the COVID-19. Rev Pediatr Aten Primaria. 2021;23:383-90.
Published in Internet: 23-11-2021 - Visits: 6838
Abstract
Introduction: the COVID-19 pandemic has driven changes in the organization of care delivery in primary care (PC) centres. The objective of our study was to describe the changes in PC paediatric care that took place in the first wave of the COVID-19 pandemic.
Material and methods: we conducted a nationwide, multicentre, retrospective, observational and descriptive study through a survey of PC paediatricians with distribution of the questionnaire in June 2020. We collected data from March 16 to May 10, 2020, divided in four 2-week periods. We asked about care delivery in these centres during this period: use of triage systems, modalities of care delivery (in person or by telephone) and volume of visits.
Results: we received 105 responses by PC paediatricians, of which 110 were considered valid. We obtained responses from paediatricians in 17 autonomous communities (72.4% in urban settings). Respondents served a cumulative population of 107 715 patients. A total of 90.5% provided remote care (38.1% did before the pandemic). Triage was conducted in all centres. The mean number of patients managed per paediatrician in each of the time intervals under study was 144, 114, 123 and 136 (compared to 277, 214, 207 and 233 in the same periods in 2019). In 88.6% of the caseloads, in-person appointments were conducted as part of the child health programme (CHP). The total number of hospital admissions for any reason in the cumulative catchment population was of 79 patients, and the number of admissions to the intensive care unit was 7. The respondents did not report any deaths.
Conclusions: in the first wave of the COVID-19 pandemic, there was a substantial increase in remote primary care paediatric visits parallel to a significant decrease in in-person visits. Triage systems were implemented. There was still substantial activity in the CHP. The number of hospital admissions and cases of serious disease was very low.
Keywords
● COVID-19 ● Demand management ● e-health ● Paediatrics ● Primary care ● TriageINTRODUCTION
In December 2019, the health authorities of China notified the World Health Organization of the detection of a series of cases of pneumonia of unknown aetiology. In a few months, the disease spread, giving rise to a pandemic.1 Research early in the pandemic established that the illness was caused by a novel coronavirus that was eventually named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), while the resulting disease was called coronavirus disease 2019 (COVID-19). In Spain, as in other countries, cases started to be detected and notified, most of mild disease (80%), but given the increasing incidence, the health care system needed to be prepared. The Spanish health authorities issued a series of recommendations regarding the access of affected patients to health care facilities, their management and followup, and epidemiological surveillance. The recommendations applied to every care level of the public and private health systems: hospitals, primary care (PC) centres and public health and preventive medicine services, all of which had to work in coordination.
With the data available to date, it was assumed that the risk of infection in children was not significant. According to the report of the National Epidemiological Surveillance Network (Red Nacional de Vigilancia Epidemiológica, RENAVE),2 based on data collected in Spain through May 10, 2020, cases in children accounted for 0.6% of the total reported. Of all children under 2 years with a diagnosis of COVID-19, 47.6% were hospitalised and 8.4% admitted to the intensive care unit (ICU). There were 3 deaths. These data were biased due to 2 aspects: they only included confirmed cases at a time when diagnostic tests were not available at the PC level, which meant that the diagnosis could only be confirmed in children managed in the hospital setting, especially those who were hospitalised. Thus, the incidence was underestimated and the severity of disease overestimated. The protocol requiring hospitalization of very young children with a confirmed diagnosis also contributed to overestimating the severity of disease in children.3
As diagnostic tests have become available at the PC level, epidemiological data have increasingly approximated actual figures. There is still a dearth of data on patients managed at the PC level in the literature, although data are already available to estimate more accurately the impact of the first wave of the COVID-19 pandemic in the paediatric population: in the RENAVE report on the cases diagnosed from May 10, 2020 through present, children under 15 years accounted for 11.9% of the total cases, and children under 2 years for 2.3% of total hospital admissions and 0.1% of total ICU admissions, with a total of 19 deaths in the entire paediatric population, corresponding to a mortality of less than 0.1%.4
These data show that in the paediatric population, the incidence of COVID-19 is similar to the incidence in adults, but the course of disease is not as severe. Nevertheless, the epidemiological role of children in the pandemic remained unknown. Their contribution to virus transmission was unknown, and another aspect that had to be taken into account was that they are patients that had to be accompanied by adults in health care visits, who could on their part be infected yet asymptomatic. This uncertainty led to organizational changes in PC centres, restricting access and reallocating health care professionals, which affected PC paediatrics clinics and their catchment populations.
The aim of our study, promoted by the Group on Infectious Diseases (GIP) of the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics, AEPap), was to analyse how PC paediatric services were organised and delivered during the first wave of the COVID-19 pandemic.
MATERIAL AND METHODS
We conducted a nationwide, multicentre, retrospective, observational and descriptive study through a survey of PC paediatricians, with distribution of the survey to all members of the AEPap (numbering 5400 as of February 2020) through the email list of members and subscribers to the PEDIAP journal5 in June 2020. The data collection period ranged from March 16, 2020, when the government declared the state of alert, to May 10 of the same year, when restrictions started to be lifted. For the purpose of analysis, we divided this period in 4 intervals of 2 weeks each. We asked about the implementation of a triage protocol in the centres and the professionals involved in triage. We also asked about the modality of care delivery (in person or by telephone) and the volume of visits, including the maximum and minimum number of patients managed per day. We compared overall demand data with data for the same time period in 2019. We performed univariate or bivariate descriptive analysis depending on the variables under study. The statistical analysis was performed with the software SPSS, version 24.
RESULTS
We considered 105 of the total 110 responses submitted by PC paediatricians valid. Of all participants, 72.4% practiced in an urban setting. Participants served a cumulative population of 107 715 patients, with a mean of 1025 patients per caseload (range, 510-1700). We received responses from paediatricians in 17 autonomous communities (ACs), and did not receive responses from Ceuta y Melilla. The response rate was highest in Madrid, Andalusia, Castilla y Leon and Aragon, which accounted for 27%, 21%, 11% and 9% of responses, respectively. Of all participants, 94.3% (n = 99) reported that their centre had a COVID-19 contingency plan. However, the date that such plans were established varied between centres. We chose as reference the dates that community transmission of the virus was established in the different regions in Spain: March 11, 2020 for Madrid and La Rioja, and March 14, 2020 for the remaining ACs. Contingency plans were established a mean of 4 days after the reference date, with a range of –9 to 108 days. The median was 2 days, with an interquartile range (IQR) of –4 to 5 days.
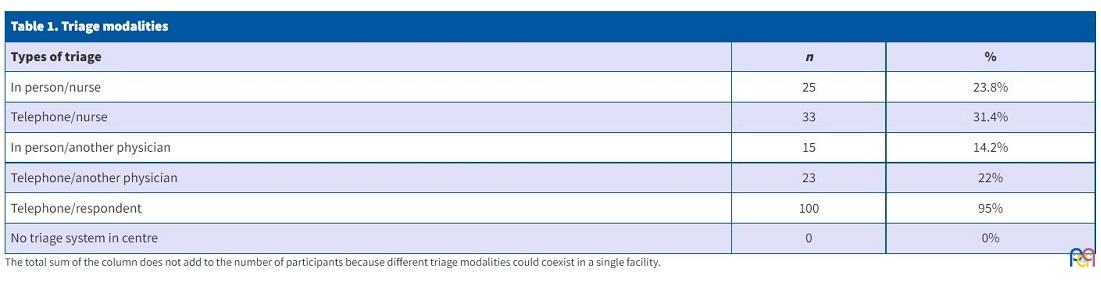
During the period under study, all centres had a triage protocol in place, implemented in person or by phone, by physicians or by nurses, frequently with a combination of the above in the same centre. Ninety-five percent of PC paediatricians reported performing telephone triage (Table 1).
| Table 1. Triage modalities | ||
|---|---|---|
| Types of triage | n | % |
| In person/nurse | 25 | 23.8% |
| Telephone/nurse | 33 | 31.4% |
| In person/another physician | 15 | 14.2% |
| Telephone/another physician | 23 | 22% |
| Telephone/respondent | 100 | 95% |
| No triage system in centre | 0 | 0% |
Four respondents reported working exclusively remotely, that is, without being physically present in the health care centre. In addition, 90.5% reported following up patients remotely, either by telephone or through other means, such as email, from the PC clinic. Before the COVID-19 pandemic, only 38% engaged in remote patient management. Fifty-three percent of respondents continued to serve their entire caseloads, while 46.5% reported that care delivery was reorganised based on patient characteristics, with the establishment of separate care pathways for patients with manifestations suggestive of COVID-19 and patients without compatible symptoms. The mean number of patients managed by each paediatrician (either in person or remotely) was 144, 114, 123 and 136 in each period, which entailed decreases of 47.8%, 46.6%, 40.6% and 41.5% compared to the same periods in 2019.
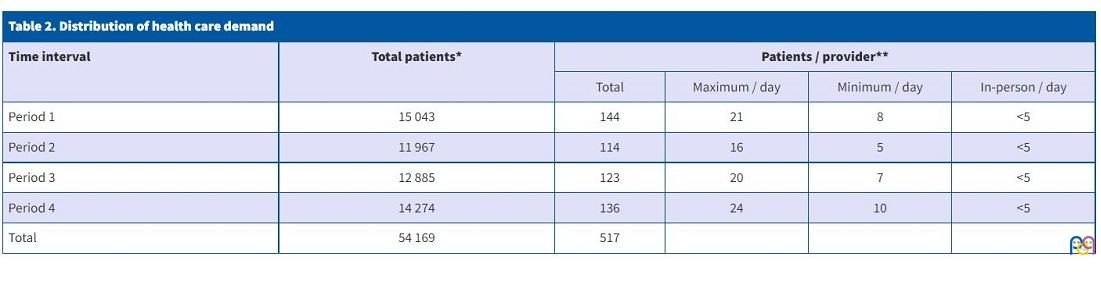
In the entire period under study, there were a total of 54 169 visits. For each of the 4 periods, the maximum mean number of patients managed per paediatrician per day was 21, 16, 20 and 24, and the minimum 8, 5, 7 and 10. The mean number of patients managed in person per paediatrician per day in 2020 was less than 5 in every time period (Table 2).
| Table 2. Distribution of health care demand | |||||
|---|---|---|---|---|---|
| Time interval | Total patients* | Patients / provider** | |||
| Total | Maximum / day | Minimum / day | In-person / day | ||
| Period 1 | 15 043 | 144 | 21 | 8 | <5 |
| Period 2 | 11 967 | 114 | 16 | 5 | <5 |
| Period 3 | 12 885 | 123 | 20 | 7 | <5 |
| Period 4 | 14 274 | 136 | 24 | 10 | <5 |
| Total | 54 169 | 517 | |||
A total of 79 patients, corresponding to 0.07% of the cumulative paediatric population served by respondents, were admitted to the paediatrics ward for any reason, including COVID-19 and other illnesses (distribution by time period: 49, 12, 11 and 7) and 7, corresponding to 0.006% of the cumulative catchment population, to a paediatric or neonatal ICU (distribution by time period: 3, 1.3 and 0).
When it came to the healthy child programme (HCP), most centres continued to carry out some of its activities, although in-person visits were pared down to a minimum, in some instances maintaining only the appointments corresponding to the first month of life. In-person care was limited to vaccination in 8.6% of the centres. All centres continued to offer primary vaccination, initially halting administration of booster doses and vaccines not funded by the public health system. When it came to healthy child appointments, 74% of centres continued scheduling appointments with both nurses and physicians. In 14% of centres, HCP visits were managed exclusively by paediatricians, and in 3% exclusively by nurses, while 8.6% discontinued HCP visits and only continued administering vaccines.
DISCUSSION
In the early months of the pandemic, it became evident that the morbidity and mortality due to COVID-19 during the first wave were significantly lower in the paediatric population compared to the other age groups.
At the start of the study, on March 16, 2020, there had been a total of 9191 COVID-19 cases reported to the RENAVE. Out of the 710 cases for which epidemiological data had been documented, 23 corresponded to children aged 0 to 14 years.6
Through May 11, 2020, when data collection ended, an additional 1409 new cases were notified in children aged 0 to 14 years, amounting to 0.6 % of the total (children under 2 years, 0.2%; children 2-4 years, 0.1%; children 5-14 years, 0.3%). The proportion of cases that resulted in hospital admission was 47.3% in children under 2 years, 25.4% in children aged 2-4 years and 18.6% in children aged 5-14 years, and the proportions admitted to the ICU were 8.4%, 2.1% and 3.5%, respectively. Three patients died.4
More recent data from the SARS-CoV-serological surveillance survey in Spain (ENE-COVID),2 whose definite results for the first wave were published on July 6, 2020 and included data for 9171 (13.5%) children under 15 years out of a total of 68 296 individuals, show an increasing trend in the incidence in the paediatric population, the perceived effects of which, however, were all but negligible. Based on this survey, the prevalence of IgG antibodies against SARS-CoV-2 in Spain in the first wave of the pandemic was estimated at 5.2% (95% confidence interval [95 CI]: 4.9- 5.5), and, in the different paediatric age groups, at: age < 1 year, 3.7%; age 1-4 years, 3.3%; age 5-9 years, 2.9%; age 10-14 years, 4.1%.
Since then, preliminary data have been published for a second phase of the survey (fourth round) comprehending the second wave, but since our study focused on the situation during the first wave, the details are out of the scope of this article.
The data collected in our study also reflected a low morbidity and mortality in children, with a low rate of hospital admission for any reason in the cumulative catchment population of 0.7% and of ICU admission of 0.006%. We also observed a decreasing trend in hospital admission through the time intervals of the study period, and while the questionnaire did not specifically ask about reasons for admission, a reasonable hypothesis would be that, early on, children given a diagnosis of COVID-19 were hospitalised even if they had mild symptoms due to the lack of knowledge of the disease, while as months went by admission was restricted to patients that required inpatient care. This hypothesis is supported by paediatric COVID-19 management protocols, which initially recommended admission in patients with mild symptoms or infants and newborns, and established more stringent admission criteria in successive updates.3
For PC paediatricians, the main impact of the pandemic in their everyday practice involved the organization of care delivery in the PC centres, both in general and at the level of their own offices.
Most respondents (94.3%) reported that the PC centre where they worked had established a contingency plan, although the timing of its institution relative to the date when the state of alert was declared varied between centres, as some established the plan before its declaration and others did it as late as 81 days after. The median time elapsed to the introduction of the plan was 2 days (IQR, -4 to 5).
We found a substantial reduction in the total number of appointments compared to the previous year, both overall, with decreases between 47.8% and 40.6% depending on the time interval, and in in-person visits, as most appointments were conducted remotely. However, depending on the AC, the reduction in the number of patients managed may have been even greater than documented, as in 2019 there were holidays and weekends in the date range under study that were workdays in 2020.
In terms of care delivery modalities, telephone care had been introduced in paediatric PC in Spain years ago, had contributed to streamlining care delivery and was perceived positively by users, but still accounted for only a small percentage of the total activity.7 In the period under study, more than 90% of PC paediatricians delivered care remotely, a very relevant finding given that 61.9% of respondents had not provided remote care before. This implementation and increase in the use of telemedicine resources in PC centres has also been observed extensively in other countries. Some authors have even reported increases of more than 86% in its use.8 For example, in the United Kingdom, 97% of providers were able to have appointments via videoconferencing and 75% offered virtual consultation compared to 25% of providers that offered remote care the previous year.9
While home confinement and the closure of schools10 achieved a decrease in morbidity, especially in terms of infectious disease, and therefore a reduction in the demand for health care, this does not explain the considerable predominance of remote care over in-person care, the latter of which has decreased substantially. It must be taken into account that in the early stages of the pandemic, efforts were made to limit the physical presence of patients in PC centres, establishing a pre-visit triage system that was mostly implemented via telephone. In Spain, there have been previous experiences with triage in PC paediatrics11,12 and recommendations issued as to its introduction and implementation,13,14 but it had not been a widespread practice until this point. The triage system is not only indispensable at present, given the need to reduce attendance of inhabitants to health care facilities. Adequate development and implementation of this system can also contribute to optimising care delivery in the future by correctly determining the type of care needed, thereby decreasing health care demand and in-person patient management. During the COVID-19 pandemic, even electronic patient self-triage tools have been developed that have exhibited a sensitivity of 87.5% to identify actual emergencies.15 In our study, we found that triage was mainly carried out by physicians, and greater involvement of nursing staff in this task would be preferable.
The sizable decrease in in-person visits following triage suggests that, in addition to administrative or bureaucratic tasks, a substantial number of clinical concerns were resolved remotely.
In the current context, these resources have achieved a reduction in health care-associated transmission, avoided unnecessary travel, allowed involvement of health care professionals who, due to different risk factors, needed to avoid in-person visits, and facilitated followup of a large number of patients.16 It has also helped mitigate the effect of interrupting the normal activity of health care services and allowed continuation of some HCP activities. Thus, remote care emerges as an alternative or, at least, an important complement to conventional care.17,18 In fact, the widespread implementation of telehealth services was one of the objectives for 2020 of the Digital Agenda for Europe.
All experiences must be used and optimised if, as it seems, the COVID-19 pandemic does not have a short-term solution, despite the vaccination campaign that is now underway. Specific documents have been published on the subject of telemedicine in paediatric care.19 Still, several authors have warned of the possible limitations of these resources in association with limited access to technology, language barriers or hearing problems. This could contribute to inequities in health.9,20 There are also concerns regarding the use of virtual resources that are not integrated in the health care system, their safety, the confidentiality of personal data, the documentation in the health records of consultations made through these resources or the lack of support by the health administration in their development.18,21 In short, as was done by the Board of Physicians of Spain with the publication in 2014 of Ética y redes sociales. Manual de estilo para médicos y estudiantes de Medicina,22 there is a pressing need for the National Health System of Spain to introduce, regulate and structure the practice of telemedicine.
When it came to the HCP and vaccination, a very high percentage—nearly 90%--of surveyed PC paediatricians continued participating in these activities, and while our survey did not specifically ask about the type of visits conducted or the vaccines administered, given the observed decrease in vaccine coverage,23 it could be inferred that the visits that were maintained were those corresponding to the youngest children.
We also ought to highlight that there were few severe cases. While there may have been others that the survey PC paediatricians did not know of, this seems unlikely, as we conducted a retrospective survey with collection of data through 1 month after the end of the period under study. In addition, most public health system databases in Spain have systems in place to dump the reports for patients managed in public hospitals in the PC electronic health records.
There are several limitations to our study. The sample of 105 professionals cannot be considered representative of the total 6622 paediatricians that are active in the PC system, based on data for 2018 of the Statistics Portal of the Ministry of Health.24 Nevertheless, it contributes information on the type of care received by a significant number of children (107 715), which may offer an approximation to the care received by the paediatric population at the PC level. As commonly observed in other surveys of PC paediatricians, we obtained the largest number of responses from Andalusia and Madrid, although in this instance there was also a substantial proportion of responses from Castilla y Leon, possibly due to this region being among the most affected by the pandemic,2 which could have motivated greater involvement by its paediatricians.
CONCLUSION
In the early phase of the COVID-19 pandemic, known as the first wave, there was a considerable decrease in demand in PC paediatrics clinics, especially for in-person appointments. The number of providers that managed patients remotely increased from 38.11% to 90.47%. Triage systems have been put in place that frequently involve PC paediatricians. The HCP has continued in most facilities, with high participation by paediatricians. There were very few severe COVID-19 cases in the caseloads of participating paediatricians. Although the frequency of seroconversion in children is nearly as high as in adults, the morbidity and mortality are substantially lower in the paediatric population.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
AC: autonomous community · AEPap: Asociación Española de Pediatría de Atención Primaria · GID: Group on Infectious Diseases of the AEPap · HCP: healthy child programme · ICU: intensive care unit · IQR: interquartile range · PC: Primary Care · RENAVE: National Epidemiological Surveillance Network of Spain · 95 CI: 95% confidence interval.
ACKNOWLEDGMENTS
We thank all paediatricians that participated for their disinterested collaboration in providing data in these particularly trying times, and the FABIS foundation in Huelva for its help with the study design, statistical analysis and approval of the project.
REFERENCES
- COVID-19 pandemic. In: European Centre for Disease Prevention and Control [online] [accessed 18/11/2021]. Available at www.ecdc.europa.eu/en/covid-19-pandemic
- Pollán M, Pérez-Gómez B, Pastor-Barriuso R, Oteo J, Hernán MA, Pérez-Olmeda M, et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. Lancet. 2020;396:535-44.
- AEPap, SEIP, SEPEAP, AEP. Manejo pediátrico en Atención Primaria del COVID-19. In: Ministerio de Sanidad [online] [accessed 18/11/2021]. Available at www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Manejo_Pediatría_ap.pdf
- Situación de COVID-19 en España. Informe n.º 30. 11 de mayo de 2020. In: Red Nacional de Vigilancia Epidemiológica en España (RENAVE) [online] [accessed 18/11/2021]. Available at https://cutt.ly/LTEKZye
- RedIRIS - Foro general sobre Pediatría [online] [accessed 18/11/2021]. Available at www.rediris.es/list/info/pediap.html
- Situación de COVID-19 en España. Informe n.º 10. 16 de marzo de 2020. In: Red Nacional de Vigilancia Epidemiológica en España (RENAVE) [online] [accessed 18/11/2021]. Available at https://cutt.ly/rTELr1k
- Monsalve Saiz M, Peñalba Citores AC, Lastra Gutiérrez S. La consulta telefónica en Atención Primaria: ¿está justificada? Rev Pediatr Aten Primaria. 2013;15:329-31.
- Bokolo JR. Use of Telemedicine and Virtual Care for Remote Treatment in Response to COVID-19 Pandemic. J Med Syst. 2020;44:132.
- Majeed A, Maile EJ, Bindman AB. The primary care response to COVID-19 in England’s National Health Service. J R Soc Med. 2020;113:208-10.
- Montiano Jorge J, Ocio Ocio I, Díez López I, Matilla Fernández A, Bosque Zabala A. ¿Qué pasaría si cerrasen las guarderías? An Pediatría (Barc). 2006;65:556-60.
- García de Ribera MC, Bachiller Luque MR, Vázquez Fernández M, Barrio Alonso MP, Hernández Velázquez P, Hernández Vázquez AM. Triaje de las urgencias pediátricas en Atención Primaria en España mediante telefonía móvil. Análisis de un modelo en una zona de salud. Rev Calidad Asistencial. 2013;28:174-80.
- Mendiola Ruiz R, Gondra Sangroniz L, Ormaechea Goiri V, Martínez Eizaguirre JM, Tadeo Múgica A, Bretos Paternain C, et al. Triaje telefónico en Atención Primaria: análisis de la implantación de un modelo. Rev Pediatr Aten Primaria. 2014;16:205-10.
- Protocolo de triaje en Pediatría de Atención Primaria. In: Osakidetza [online] [accessed 22/11/2021]. Available at www.osakidetza.euskadi.eus/contenidos/informacion/gidep_epdt/es_def/adjuntos/GIDEP_Triaje_AP.pdf
- Álvarez de Laviada Mulero T, Martínez Pons M, Mínguez Verdejo R, Sebastián Barberán V, Serrano Poveda E, Suárez Vicent E, et al. Recomendaciones para la atención de urgencias y consultes no demorables en la consulta pediátrica de Atención Primaria. Informe GATPAP. In: AEPap [online] [accessed 22/11/2021]. Available at www.aepap.org/sites/default/files/noticia/archivos-adjuntos/informe_gatpap.pdf
- Judson TJ, Odisho AY, Neinstein AB, Chao J, Williams A, Miller C, et al. Rapid Design and Implementation of an Integrated Patient Self-Triage and Self-Scheduling Tool for COVID-19. J Am Med Inform Assoc JAMIA. 2020;27:860-6.
- Vidal-Alaball J, Acosta-Roja R, Pastor Hernández N, Sánchez Luque U, Morrison D, Narejos Pérez S, et al. Telemedicine in the face of the COVID-19 pandemic. Aten Primaria. 2020;52:418-22.
- Fagherazzi G, Goetzinger C, Rashid MA, Aguayo GA, Huiart L. Digital Health Strategies to Fight COVID-19 Worldwide: Challenges, Recommendations, and a Call for Papers. J Med Internet Res. 2020;22:e19284.
- Bravo Acuña J, Merino Moína M. Uso de nuevas tecnologías en la comunicación con los pacientes, su utilidad y sus riesgos. An Pediatría (Barc). 2020;92:251-2.
- Burke BL Jr, Hall RW; Section on Telehealth Care. Telemedicine: Pediatric Applications. Pediatrics. 2015;136:e293-e308.
- Katzow MW, Steinway C, Jan S. Telemedicine and Health Disparities During COVID-19. Pediatrics. 2020;146:e20201586.
- Muñoz Fernández L, Díaz García E, Gallego Riestra S. Las responsabilidades derivadas del uso de las tecnologías de la información y comunicación en el ejercicio de las profesiones sanitarias. An Pediatría (Barc). 2020;92:307.e1-307.e6.
- Gutiérrez Fernández R, Jiménez Aldasoro M, Lalanda Sanmiguel M, Olalde Quintana R, Satué Vallvé B, Taberner Ferrer, R et al. Ética y redes sociales. Manual de estilo para médicos y estudiantes de medicina. Organización Médica Colegial; 2016.
- Moraga FA. Las vacunaciones caen durante la pandemia. Adolescere. 2020;VIII.
- Consulta Interactiva del SNS. In: Portal Estadístico. Ministerio de Sanidad [online] [accessed 22/11/2021]. Available at https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/I/sistema-de-informacion-de-atencion-primaria-siap/resumen-grafico-siap/centros-y-profesionales
Comments
This article has no comments yet.