

Vol. 23 - Num. 91
Original Papers
Relationship between the use of health resources and psychosocioeconomic aspects in Primary Care
Raquel Martín Martína, Marciano Sánchez Bayleb
aPediatra. CS Párroco Julio Morate. Madrid. España.
bPediatra. Fundación para la Investigación, Estudio y Desarrollo de la Salud Pública. Madrid. España.
Correspondence: R Martín. E-mail: raquelmartin333@hotmail.com
Reference of this article: Martín Martín R, Sánchez Bayle M. Relationship between the use of health resources and psychosocioeconomic aspects in Primary Care. Rev Pediatr Aten Primaria. 2021;23:239-46.
Published in Internet: 12-07-2021 - Visits: 4823
Abstract
Introduction: the aim of our study was to analyse the influence of family socioeconomic and psychological factors on the demand and use of health resources in paediatric consultations in Primary Care.
Methods: descriptive observational study carried out using questionnaires collected over a period of 1 year. Questionnaires were collected from children between 1 month and 14 years old, belonging to 2 urban Primary Care clinics in Madrid. The raw data was analysed, and comparisons between groups and multivariate analysis were performed.
Results: we compared 434 questionnaires. The number of total consultations was higher in younger patients (p = 0.001) and in those whose parents presented high levels of anxiety (p = 0.001). Families with all their members in unemployed presented anxiety (OR: 5.85; IC 95: 2.567-13.341; p <0.0001) and depression (OR: 6.250; IC 95: 2.647-14.760; p <0.0001) levels higher than the rest. Laboratory and imaging test were higher in children with chronic disease (OR: 3.84; IC 95: 2.09-7.07; p <0.0001) and high level of anxiety in parents (OR: 2.78; IC 95: 1.46-5.28; p = 0.02). Drugs use was higher in children with chronic disease (OR: 3.15; IC 95: 1.60-6.19; p = 0.001) and lower in older children (OR: 0.927; IC 95: 0.87-0.98; p = 0.014).
Conclusions: hyper-attendance and drug consumption in general and antibiotics in particular, as well as the request for imaging and laboratory test, is directly related to the high level of anxiety in the parents and the presence of chronic disease in children and inversely with the age. It would be advisable to detect and, if possible, intervene in cases of high parental anxiety in order to try to reduce the consumption of health resources.
Keywords
● Health resources ● Socioeconomic levelINTRODUCTION
The National Health System (NHS) of Spain is considered to be one of the best in the world, and within it, primary care (PC) is rated highly by the population in health care quality surveys.1,2 However, despite this positive perception, PC is currently in crisis.3 There have been significant political and economic changes in Spanish society in recent years that have been detrimental to the various resources that allowed the NHS to excel.4,5
There is a substantial amount of literature on the subject of frequent attenders in primary care.6-8 This is a complex phenomenon with multiple causes: on one hand, the near lack of economic barriers to access, which fosters equity in medical care but, on the other hand, in a society with consumeristic tendencies, turns health care into additional services and goods available for consumption,9,10 leading to the medicalization of everyday life, a trend that is in part facilitated by the system itself, which contributes to it,11 in addition to health prevention, promotion and education failing to prevent the overuse of health care resources, despite the efforts made by health professionals on these areas.12
Few studies have analysed the different factors involved in the use of health care resources that may lead to overuse in the field of paediatrics.13
It must be taken into account that appropriate budget planning and implementation by policymakers and health professionals is essential to the sustainability of the health care system.
Knowing the health care needs of the population is also indispensable for the purpose of planning and managing budgets, and these needs are partly determined by the psychological and socioeconomic factors. The aim of our study was to assess the impact of psychological and socioeconomic factors on health care utilization in the catchment population of 2 PC paediatrics clinics.
MATERIAL AND METHODS
We conducted an observational descriptive study by analysing data obtained from a questionnaire completed by the parents of 434 children aged 1 month to 14 years that visited 2 paediatric clinics in 2 primary care centres in the city of Madrid, Spain. The questionnaire had been validated in a pilot study (reliability: Cronbach α, 0.768, p <0.0001; validity: confirmatory factor analysis and item-test correlation coefficient). The total of health care cards included in the 2 paediatrics caseloads in the age range under study corresponded to 2580 children, and we offered participation in the survey between January 2018 and August 2019 to a sample selected at random from all the children that had a PC paediatrics visit, whether scheduled or on-demand.
We collected data on the following variables: child age and sex, parental age and country of origin, household variables including whether the parents lived together or apart and household income, number of visits to the PC centre, emergency departments or after-hours urgent care clinics (UCCs), ordered imaging or laboratory tests and referrals to medical specialists, prescription of antibiotics and other drugs and administration of vaccines not funded by the public health care system. We also asked parents to complete the Goldberg anxiety and depression scale,14 a screening tool used to detect these mental health disorders. The global score has a sensitivity of 83% and a specificity of 82%, it is administered in interview mode, and the cut-off values are 4 or more points for the anxiety subscale and 2 or more points for the depression subscale. The scale was developed to identify probable cases and not for final diagnosis. We collected data on visit frequency from electronic health records.
When it came to household income, we established 2 groups: household income greater or less than €1000.
The primary outcomes were the number of visits to primary care centres, UCCs and hospital emergency departments and the total number of medical visits. Other endpoints analysed in the study were performance of imaging or laboratory tests, referrals to medical specialists and drug prescription (antibiotics and other drugs).
The statistical analysis was performed with the software SPSS version 15.0. We summarised quantitative data as mean and standard deviation (SD), and qualitative data as absolute frequencies and percentages. We calculated 95% confidence intervals (95 CI). We compared quantitative data using the Mann-Whitney U test after determining they did not fit a normal distribution (Kolmogorov-Smirnov test). We compared qualitative data by means of the chi square test, with calculation of odds ratios. P-values of less than 0.05 were considered statistically significant. We conducted a multivariate analysis by means of binary logistic regression and multiple linear regression, starting with the full model and using backward elimination until only variables with a statistically significant association remained.
RESULTS
We collected data for 434 patients, of who 200 (46.08%) were male and 234 (53.91%) female, with a mean age of 3.68 years (range: 1 month-14 years; SD: 3.36). The mean maternal age was 36.58 years (SD: 6.29) and the mean paternal age was 38.87 (SD: 7.24). The mean number of children of the respondent was 1.64 (SD: 0.76), and 261 of the patients (60.1%) were first-born children. Of all patients, 49 (11.29%) lived in single-parent households and 197 (45.39%) had at least 1 immigrant parent. The household income was less than €1000 in 82 cases (18.89%) and more in 352 (81.10%). In 26 cases (5.99%), both parents were unemployed.
In the Goldberg scale, the mean score in the anxiety subscale was 1.10 (SD: 2.71) and the mean score in the depression subscale was 0.70 (SD: 2.14). There were 64 respondents (14.74%) with scores of 4 points or greater in the anxiety subscale and 55 (12.67%) with scores of 2 points or greater in the depression subscale.
The mean total number of medical visits was 2.22 (SD: 1.60); 87 patients (20.09%) were referred to medical specialists; antibiotics were prescribed to 92 patients (21.19%); 286 patients (65.98%) had drug prescriptions; 47 (10.82%) had undergone imaging tests and 65 (14.97%) laboratory tests; 275 families (63.36%) chose to pay for vaccines that were not included in the routine immunization schedule of the Community of Madrid and 68 patients (15.66%) had chronic diseases. Table 1 summarises the epidemiological characteristics of the sample.
| Table 1. Epidemiological characteristics of the sample |
|---|
| Age of patient, years: mean 3.68 (SD: 3.36) |
| Maternal age, years: mean 36.58 (SD: 6.29) |
| Paternal age, years: mean 38.87 (SD: 7.24) |
| Number of children: mean 1.64 (SD: 0.76) |
| Single-parent households: n = 49 (11.29%) |
| Immigrant families: n = 197 (45.39%) |
| Monthly household income: > €1000, 82 (18.89%); > €1000, 352 (81.10%) |
| Goldberg scale scores: anxiety subscale: mean 1.10 (SD: 2.71); depression subscale: mean 0.70 (SD: 2.14); score ≥4 in the anxiety subscale, n = 64; score ≥2 in the depression subscale, n = 55 |
| Total visits: mean 2.22 (SD: 1.60); visits to primary care centre: mean 1.64 (SD: 1.02); urgent visits: mean 0.49 (SD: 0.98) |
| Referrals to speciality care: n = 87 (20.09%) |
| Use of antibiotics: n = 92 (21.19%) |
| Use of pharmaceuticals: n = 286 (65.89%) |
| Imaging: n = 47 (10.82%) |
| Laboratory tests: n = 65 (14.97%) |
| Privately funded vaccines: n = 275 (63.36%) |
| Patients with chronic disease: n = 68 (15.66%) |

Table 2 presents the Spearman correlation coefficients for the associations between the number of visits to primary care centres, emergency and urgent care services and total visits, on one hand, and the scores on the depression and anxiety subscales in the Goldberg scale and the age in years of participants, on the other, which show a significant correlation in every case except between the depression subscale score and the number of urgent visits.
| Table 2. Spearman correlation coefficient for the association between the number of visits (total, to primary care centre, to urgent care services) and patient age and scores in anxiety and depression subscales in the total sample | |||
|---|---|---|---|
| Anxiety score | Depression score | Age in years | |
| Primary care visits | 0.158 (p = 0.001) | 0.113 (p = 0.018) | 0.141 (p = 0.003) |
| Urgent care visits | 0.149 (p = 0.002) | 0.059 (p = 0.220) | 0.110 (p = 0.02) |
| Total visits | 0.210 (p <0.0001) | 0.137 (p = 0.004) | 0.158 (p = 0.001) |

Table 3 summarises the results of the multivariate linear regression analysis for the total number of medical visits, which show that the only associations that continued to be statistically significant were the positive association with the anxiety subscale score and the negative association with age.
| Table 3. Results of multiple linear regression analysis for the total number of visits (data for variables with a significant association) | |||
|---|---|---|---|
| Beta | 95 CI | p | |
| Age | -0.071 | -0.114 to -0.028 | 0.001 |
| Anxiety score | 0.162 | 0.109 to 0.215 | <0.0001 |

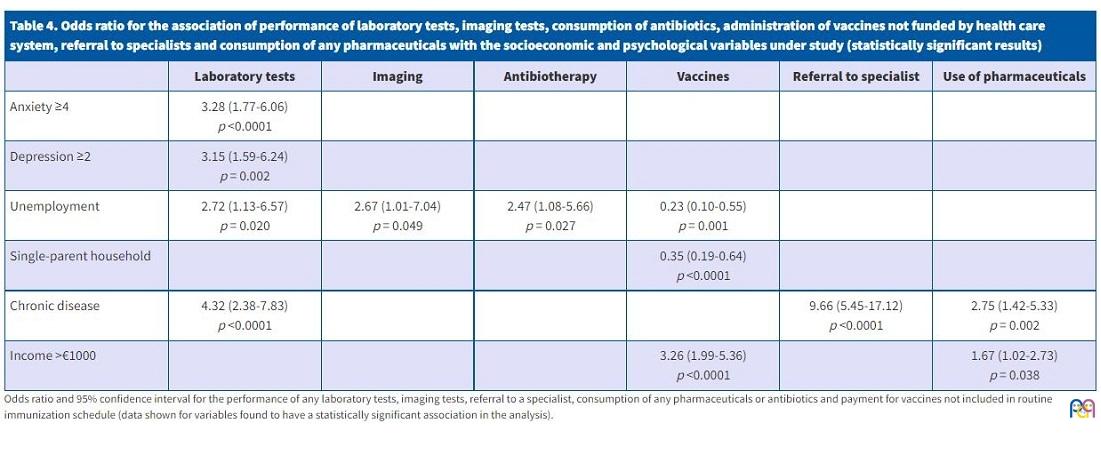
Table 4 presents the odds ratios (ORs) obtained for the performance of laboratory tests of any kind and the purchase of vaccines not funded by the public health system, showing that the performance of laboratory tests was more likely in children that had chronic disease or of parents who were unemployed or with anxiety scores of 4 points or greater or depression scores of 2 or greater, while the purchase of vaccines not publicly funded was significantly more frequent in patients from households with incomes greater than €1000 (OR: 3.267; 95 CI: 1.990 to 5.362; p <0.0001) and less frequent in children of unemployed parents or living in a single-parent household. There was also evidence that use of pharmaceuticals was more frequent in patients with chronic diseases (OR: 2.75; 95 CI: 1.42 to 5.33; p = 0.002) or from households with incomes greater than €1000 (OR: 1.67; 95 CI: 1.01 to 7.04; p = 0.049), while antibiotic consumption was more frequent in patients with unemployed parents (OR: 2.47; 95 CI: 1.08 to 5.66; p = 0.027).
| Table 4. Odds ratio for the association of performance of laboratory tests, imaging tests, consumption of antibiotics, administration of vaccines not funded by health care system, referral to specialists and consumption of any pharmaceuticals with the socioeconomic and psychological variables under study (statistically significant results) | ||||||
|---|---|---|---|---|---|---|
| Laboratory tests | Imaging | Antibiotherapy | Vaccines | Referral to specialist | Use of pharmaceuticals | |
| Anxiety ≥4 | 3.28 (1.77-6.06) p <0.0001 |
|||||
| Depression ≥2 | 3.15 (1.59-6.24) p = 0.002 |
|||||
| Unemployment | 2.72 (1.13-6.57) p = 0.020 |
2.67 (1.01-7.04) p = 0.049 |
2.47 (1.08-5.66) p = 0.027 |
0.23 (0.10-0.55) p = 0.001 |
||
| Single-parent household | 0.35 (0.19-0.64) p <0.0001 |
|||||
| Chronic disease | 4.32 (2.38-7.83) p <0.0001 |
9.66 (5.45-17.12) p <0.0001 |
2.75 (1.42-5.33) p = 0.002 |
|||
| Income >€1000 | 3.26 (1.99-5.36) p <0.0001 |
1.67 (1.02-2.73) p = 0.038 |
||||
Compared to the rest of the sample, respondents in families in which both parents were unemployed were more likely to have anxiety scores of 4 or greater (OR: 5.85; 95 CI: 2.567 to 13.341; p <0.0001) and depression scores of 2 or greater (OR: 6.250; 95 CI: 2.647 to 14.760; p <0.0001).
Table 5 shows the results of the logistic regression analysis of the performance of laboratory tests, which was positively associated with a score of 4 or greater in the anxiety subscale of the Goldberg scale and with the presence of chronic disease in the patient.
| Table 5. Results of the logistic regression analysis of the performance of at least 1 laboratory test (data for variables with a significant association in the model) | |||
|---|---|---|---|
| OR | 95 CI | p | |
| Anxiety score ≥4 | 2.78 | 1.46-5.28 | 0.02 |
| Chronic disease | 3.84 | 2.09-7.07 | <0.0001 |

Table 6 shows the results of the logistic regression analysis of the use of pharmaceuticals, which revealed a positive association with chronic disease and a negative association with age.
| Table 6. Results of the logistic regression analysis of the use of at least 1 pharmaceutical (data for variables with a significant association in the model) | |||
|---|---|---|---|
| OR | 95 CI | p | |
| Chronic disease | 3.15 | 1.60-6.19 | 0.001 |
| Age | 0.927 | 0.87-0.98 | 0.014 |

DISCUSSION
The health care needs of the population do not always translate to correct use of the available resources.15,16 Development of health care policy requires an understanding of the determinants of health, and it is known that individual health is closely related to socioeconomic status in the society that the individual belongs to, and in particular, child health depends largely on parental socioeconomic status.17,18 At present, there are vast social inequalities, and there is a social gradient in health that runs along the socioeconomic spectrum: individuals in the most disadvantaged social classes have worse health and shorter lifespans and receive care of lower quality.19
There is a growing interest in the social determinants that contribute to health care utilization in the general population reflected in an increasing number of studies on the subject.20-22
Providing care on demand has a high economic cost. The number of visits to PC paediatricians and paediatric specialists is an indicator of health care utilization. In our study, we found that parents with high levels of anxiety made more visits, which corroborated the results of a previous study recently published by our group.23 Levels of anxiety and depression were higher in households in which both parents were unemployed, single-parent households and households where a child had chronic disease. There is a substantial body of evidence evincing the association between the frequency of paediatric care visits and parental levels of anxiety and depression.24,25 Our study contributed something new by applying the Goldberg scale, which is easy to use at the PC level, as it can provide clues of the psychological condition of parents in terms of anxiety and depression levels in a few minutes; we also found that the frequency of visits was inversely associated with patient age, that is, the younger the patient, the more frequent the visits and vice versa, something that had already been described by other authors.26 The presence of chronic disease in children entails a greater use of pharmaceuticals, imaging tests and laboratory tests. Patients who had 2 unemployed parents were more likely to receive antibiotics.27 Arias Álvarez et al.28 found similar results regarding the use of pharmaceuticals and the frequency of medical visits. We did not find an association between the use of health care resources and parental country of origin, in agreement with the findings of Arias et al.
When it came to the referrals to medical specialists performed in the caseloads under study, we found a positive association with patient age.29
The purchase of vaccines not funded through the routine immunization programme was mainly observed in higher-income households.
The sample under study provided ample representation of the immigrant population, as 45.39% of the patients in the sample had at least 1 parent from another country. We found no evidence of greater health care utilization by this group compared to Spanish nationals, which was consistent with the findings published by Gimeno-Feliu et al.30 The immigrant subset in our study shared all analysed characteristics with the immigrant population described in our previous study.31 In Spain, the immigrant population generally comes from low-income countries, and despite its anticipated contribution to the sustainability of the welfare state,32 the fact is that immigrants generally belong to the most disadvantaged segments of the population, deserving of special attention in the allocation of resources to keep from widening the existing gap between socioeconomic levels.
There are limitations to our study, chiefly the size of the sample, which was selected from the caseloads of only 2 centres and was not representative of the population of the Community of Madrid, and the collection of data through a questionnaire, which may lead to errors in documentation and recall bias.
Given the complexity and relevance of this issue, further studies would be useful, especially in larger samples, since, as our results once again reaffirm the multifactorial basis of health care utilization, which on one hand involves health care providers33-35 but on the other depends on the characteristics of the population covered by the services, with unemployment and a household income under €1000 being particularly important. Our study evinces the extreme vulnerability of the most disadvantaged segments of the population and the importance of psychological and socioeconomic factors on health. Adequate administration of health care resources is key to protect the population from what Benach et al.36 refer to as the worst epidemic of the XXI century: health care inequity.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
OR: odds ratio · NHS: National Health System · PC: Primary care · SD: standard deviation · UCC: urgent care centre · 95 CI: 95% confidence interval.
REFERENCES
- Murillo C, Saurina C. Medida de la importancia de las dimensiones de la satisfacción en la provisión de servicios de salud. Gac Sanit. 2013;27:304-9.
- La Atención Primaria de Salud en 2025. In: Organización Médica Colegial de España. Consejo General de Colegios Oficiales de Médicos. Documentos 2017 [online] [accessed 06/07/2021]. Available at www.cgcom.es/sites/default/files/atencion_primaria_2025/19/
- Legido-Quigley H, Urdaneta E, González A, La Parra D, Muntaner C, Álvarez-Dardet C, et al. Erosion of universal health coverage in Spain. Lancet. 2013;382:1977.
- Mellado MJ. La AEP, determinante en los cambios profesionales, epidemiológicos, socioculturales y medioambientales que impactaran en la salud de los niños del país. An Pediatr (Barc). 2019;90:338-41.
- La crisis, los niños y los pediatras. Noviembre 2012. In: Asociación Española de Pediatría [online] [accessed 06/07/2021]. Available at www.aeped.es/sites/default/files/encuesta_aep.pdf
- Herranz Jordán B, Jiménez García JJ. Hiperfrecuentación en urgencias pediátricas. An Pediatr (Barc). 2017;87:121.
- Rivas García A, Manrique Martín G, Butragueño Laiseca L. Hiperfrecuentación y la oferta de atención pediátrica. An Pediatr (Barc). 2017;87:123.
- Fernández Alonso C, Aguilar Mulet M, Romero Pareja R, Rivas García A, Fuentes Ferrer ME, González Armengol JJ. Hiperfrecuentacion en Atención Primaria e hiperfrecuentadores en urgencias. Aten Primaria. 2018;50:222-7.
- Estadística de Gasto Sanitario Público, principales resultados. In: Ministerio de Sanidad y Consumo 2018 [online] [accessed 06/07/2021]. Available at www.mscbs.gob.es/estadEstudios/estadisticas/docs/EGSP2008/egspPrincipalesResultados.pdf
- Segura Benedicto A, Giner Ruiz V. El consumo sanitario inapropiado y la trivialización de la medicina. Aten Primaria. 2013;45:274-7.
- Orueta Sánchez R, Santos Rodríguez C, González Hidalgo E, Fagundo Becerra EM, Alejandre Lázaro G, Carmona de la Morena J, et al. Medicalización de la vida (I). Rev Clin Med. 2011;4:150-61.
- Piñeiro Pérez R, Carabaño Aguado I. Hiperfrecuentación en urgencias. Experiencia y fracaso de una consulta de educación sanitaria. An Pediatr (Barc). 2017;87:362.
- Priego Álvarez HR (dir.). Consumo en Salud. Análisis Mercadológico del comportamiento del consumidor sanitario. In: Universidad Autónoma de Barcelona [online] [accessed 06/07/2021]. Available at www.tdx.cat/handle/10803/4614#page=1
- Lobo A, Montón C, Campos R, García-Campayo J, Pérez Echevarria MJ. Detección de morbilidad psíquica en la práctica médica. El nuevo instrumento EADG. Zaragoza: Luzán; 1993.
- Fundación Foessa. Informe sobre exclusión y desarrollo social en Madrid. In: Cáritas [online] [accessed 06/07/2021]. Available at www.caritasmadrid.org/viii-informe-foessa-sobre-exclusion-y-desarrollo-social-en-la-comunidad-de-madrid-2019
- Llano Ortiz JC. 9º Informe AROPE (2019). El estado de la pobreza. Seguimiento del indicador de pobreza y exclusión social en España [online] [accessed 06/07/2021]. Available at www.eapn.es/estadodepobreza/
- Coduras Martínez A, del Llano Señaris JE. La Sanidad Española en cifras. In: Asociación Española de Enfermería de Salud Mental [online] [accessed 06/07/2021]. Available at www.aeesme.org/wp-content/uploads/2019/05/Sanidad-espanola-en-cifras-2018.pdf
- Sastre Paz M, Terol Claramonte M, Clara Zoni A, Esparza Olcina MJ, del Cura González MI. Tomando conciencia de las desigualdades sociales en la salud de la población infantil. Aten Primaria. 2016;18:203-8.
- Determinantes sociales de la salud. Comisión sobre Determinantes Sociales de la Salud. 14. In: World Health Organization [online] [accessed 06/07/2021]. Available at www.who.int/social_determinants/es/
- Jiménez Rubio D, Ortega Ortega M. Salud y posición socioeconómica: evidencia empírica reciente en el panorama internacional y en España. Rev Estud Empres. 2014;1:40-5.
- Stringhini S, Carmeli C, Jokela M, Avendaño M, Muenning P, Guida F, et al. Socioeconomic status and the 25 x 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1.7 million men and women. Lancet. 2017;389:1229-37.
- Actividad y calidad de los servicios sanitarios. Informe anual del Sistema Nacional de Salud 2017. In: Ministerio de Sanidad, Consumo y Bienestar Social [online] [accessed 06/07/2021]. Available at www.mscbs.gob.es/estadEstudios/estadisticas/sisInfSanNHS/tablasEstadisticas/InfNHS2017.htm
- Martín Martín R, Sánchez Bayle M, Teruel de Francisco C. Aspectos psicosociales relacionados con la hiperfrecuentación en las consultas pediátricas de Atención Primaria. An Pediatr (Barc). 2019;90:26-31.
- Montalbán Sánchez J. Relación entre ansiedad y dinámica familiar. Aten Primaria. 1998;21:29-34.
- Tapia Collados C, Gil Guillen V, Orozco Beltrán D. Influencia de la ansiedad materna en la frecuentación de las consultas de Atención Primaria. Aten Primaria. 2005;36:167-8.
- Sandín Vázquez M, Conde Espejo P. Hiperfrecuentación: percepción de los profesionales de Atención Primaria sobre la influencia de factores sociales y de organización del entorno sanitario. Rev Calid Asist. 2011;26:256-63.
- García Vera C, Albañil Ballesteros MR. Prescripción de antibióticos en la Atención Primaria pediátrica: una responsabilidad compartida. An Pediatr (Barc). 2018;89:195-6.
- Arias Álvarez MA, Sánchez Bayle M, Gancedo García C, Martín Martín R, Estepa Soto MR, Díaz Martínez ME. Nivel socioeconómico y consumo de recursos sanitarios en Atención Primaria. An Pediatr (Barc). 2004;61:292-7.
- Contreras Balada N, Gilbert Agulló A, Linares Muñoz JM, Ponce Villacreces MC, Casamada Humet N, Sauvalle Soler M. Análisis de las derivaciones a la Atención Especializada desde la consulta de Atención Primaria. Rev Pediatr Aten Primaria.2015;17:e13-e20.
- Gimeno-Feliu LA, Macipe-Costa RM, Dolsac I, Magallón-Botaya R, Luzón L, Prados-Torres, et al. Frecuentación de la población inmigrante versus autóctona en Atención Primaria: ¿Quién consume más servicios? Aten Primaria. 2011;43:544-50.
- Martín Martín R, Sánchez Bayle M, Gancedo García C, Teruel de Francisco MC, Coullaut López A. Las familias de la crisis en las consultas pediátricas de Atención Primaria: estudio descriptivo observacional. An Pediatr (Barc). 2016;84:189-94.
- Bruquetas Callejo M, Moreno Fuentes F. Inmigración y Estado de Bienestar en España. Colección Estudios Sociales. Obra Social La Caixa. In: Fundación de la Lengua Española [online] [accessed 06/07/2021]. Available at www.fundacionlengua.com/extra/descargas/des_36/ARTICULOS/volumen-31-de-la-coleccion-de-estudios-sociales-i-inmigracion-y-estado-de-bienestar-en-espana-i.pdf
- Compromisos de Gobierno 2019-2023. In: Comunidad de Madrid [online] [accessed 06/07/2021]. Available at www.comunidad.madrid/transparencia/compromisos-gobierno-2019-2023
- Pavo García MR, Martínez González C. Recomendaciones para “no hacer” en Pediatría. Rev Pediatr Aten Primaria. 2018;20:291-5.
- Ruiz-Canela Cáceres J. Dejar de hacer, pero elegir con prudencia. In: AEPap (ed). Curso de Actualización Pediatría 2018. Madrid: Lúa Ediciones 3.0; 2018. p. 309-15.
- Benach J, Vergara M, Muntaner C. Desigualdad en salud: la mayor epidemia del siglo XXI. Papeles de relaciones sociales y cambio global. Papeles. 2008;103:29-40..
Comments
This article has no comments yet.