

Vol. 23 - Num. 90
Original Papers
Rational use of antibiotics in acute pharyngotonsillitis
aFarmacéutica. Servicio de Farmacia de Atención Primaria. Dirección de Atención Primaria Sector Teruel. Teruel. España.
Correspondence: C Pérez . E-mail: cperezd@salud.aragon.es
Reference of this article: Pérez Diez C. Rational use of antibiotics in acute pharyngotonsillitis. Rev Pediatr Aten Primaria. 2021;23:155-62.
Published in Internet: 18-06-2021 - Visits: 6032
Abstract
Objective: to assess whether a pharmaceutical education intervention achieved a reduction and improvement in the prescription of antibiotics for management of paediatric acute pharyngitis (PAP).
Material and methods: we conducted a pre-post intervention study. We analysed the prescription of systemic antibiotics (J01) associated with diagnoses corresponding to CIAP codes for streptococcal pharyngitis-tonsillitis (R72), acute pharyngitis (R74) and acute tonsillitis (R76) before and after a pharmaceutical education intervention on primary care (PC) paediatricians. We calculated the percentage of antibiotic prescriptions corresponding to first-line antibiotics (penicillin V, penicillin G or amoxicillin) associated with CIAP code R72 and CIAP codes R74-R76. The pharmaceutical education intervention consisted of a training workshop and clinical sessions.
Results: the prescription of systemic antibiotics decreased significantly in the post-intervention period compared to the pre-intervention period (44.1% versus 46.2%; p = 0.014). There was a significant increase in the percentage of first-line antibiotic prescriptions out of the total prescriptions associated with CIAP code R72 (84.3% versus 57.6%; p = 0.000) and a decrease in the proportion of prescriptions of amoxicillin-clavulanic acid (13.6% versus 22.9%; p <0.001) and azithromycin (1.0% versus 11.3%; p <0.001) over the total prescriptions associated with CIAP code R72.
Conclusions: there was a decrease in antibiotic prescription by PC paediatricians with improvement in the prescription of first-line agents for PAP.
Keywords
● Acute pharyngitis ● Antibacterial agents ● Drug resistance, microbial ● Early management education ● Public HealthINTRODUCTION
The generalised and unnecessary prescription of antibiotics is contributing to the emergence of antimicrobial resistances, a significant problem that jeopardises the effectiveness of these drugs.1 Concerns regarding the rational use of antibiotics have led to the launching of antimicrobial stewardship programmes in the autonomous community (AC) of Aragon in Spain, following the guidelines established in the National Strategy on Antimicrobial Resistance (Plan Nacional de Resistencia a los Antimicrobianos, PRAN). In adherence with these guidelines, qualitative and quantitative indicators were developed to monitor antibiotic use with the aim of reducing inadequate utilization and promote prescription of narrow-spectrum antibiotics. Educational strategies aimed at improving awareness regarding antibiotic use in the community and targeted interventions aimed at changing the behaviour of health professionals through training, consultation, audits, and electronic prescription tools can help improve antibiotic prescription practices.2
In the field of paediatrics, antibiotic prescription is most frequently associated with episodes of acute pharyngitis (AP), which accounts for 22.6% of the total.3 However, most cases of AP have a viral aetiology, and the proportion of cases caused by streptococcus in children is approximately 13%.4 The unnecessary prescription of antibiotics can produce side effects on the patient, selection of resistant pathogens and unnecessary health care costs. Antibiotherapy for management of AP caused by Streptococcus pyogenes is only indicated if the bacterial aetiology is confirmed by rapid antigen detection test (RADT) or culture)5,6 and is the first-line treatment in children that are not allergic to oral penicillin because there is no evidence of resistance (susceptibility in 100% of isolates) and due to its narrow spectrum it is less likely to cause resistance in other pathogens.
The aim of our study was to assess whether a pharmaceutical education intervention in primary care (PC) paediatricians can improve antibiotic prescription in paediatric cases of AP, reduce antibiotic use and optimise the use of first-line antibiotic agents for management of acute streptococcal pharyngitis (ASP).
MATERIAL AND METHODS
Study design: pre-post intervention study.
Setting
The universe consisted of PC paediatricians in the Teruel health care area. In 2018, this health care area covered a population of 74 128 inhabitants (of who 12.8% were children aged 0-14 years), served by 10 PC paediatricians.
Sample selection
We emailed the PC paediatricians of the Teruel health care area (n = 10) to invite them to a face-to-face training. There were no changes in the PC paediatricians on staff during the period under study, so that the same paediatricians provided care in both study periods (pre- and post-intervention), a condition that we deemed necessary to be able to compare the results.
Intervention
The intervention consisted of a single workshop, titled “Optimization of Antibiotic Prescription in Paediatrics” (“Opt”, delivered by the PC pharmacist), attended by 2 PC paediatricians and 10 family physicians employed in the Teruel health care area. The training took place on May 29, 2018, lasted 3 hours, and was accredited by the board that oversees continuing education in health care professions in Aragón for a total of 0.4 credits. The content was developed following a review of the current evidence to provide recommendations on the diagnostic criteria and management of paediatric AP, and included clinical cases used to guide the symptomatic treatment of viral infections considered to be benign and self-limited; recommending delay of antibiotic prescription and promoting the use of RADT as a diagnostic tool to guide prescription of antibiotherapy for ASP. The training materials were submitted by email to the 8 PC paediatricians that were unable to attend the face-to-face session. Since June 1, 2018, every primary care team (PCT) in the health care area (in paediatrics clinics, emergency departments or urgent care centres [UCCs]) has access to the RADT, distributed by the Primary Care Pharmacy Department (PCPD), in addition to a protocol for establishing eligibility for the test based on the Centor criteria.7
Study variables
We analysed active electronic prescriptions for systemic antibacterials (J01 therapeutic subgroup in the Anatomical Therapeutic Chemical [ATC] classification) associated with International Classification of Primary Care (ICPC)8 codes for strep throat (R72), acute pharyngitis/acute upper respiratory infection (R74) and acute tonsillitis (R76) with the cut-off dates of May 1, 2018 (pre-intervention period) and May 1, 2020 (post-intervention period). Each unit in the analysis corresponded to a single electronic prescription and one care episode or ICPC code. The training emphasised that in patients with manifestations of acute pharyngitis, the ICPC code R72 should only be used if the patient met at least 2 Centor criteria and had a positive RADT; using code R74 in case of viral pharyngitis (< 2 Centor criteria or ≥2 Centor criteria and negative RADT) and code R76 in cases of suspected bacterial infection based on clinical criteria (2 Centor criteria or ≥3 Centor criteria) and RADT not performed or not available.7 Although antibiotherapy should be prescribed in the latter cases (clinical suspicion of bacterial infection in the absence of RADT results), we considered antibiotic prescriptions associated with ICPC codes R74 and R76 inappropriate for the purpose of the comparative analysis, as all PCTs in the Teruel health care area had access to the RADT.
We analysed sociodemographic variables (sex, age); the total number of episodes (n) with ICPC codes R72, R74 and R76 associated with active prescriptions of systemic antibiotics (J01) pre and post intervention; variables related to the rational use of antibiotics pre and post intervention (percentage of prescriptions of first-line antibiotics associated with ICPC code R72, calculated as the quotient of the prescriptions of penicillin V [J01CE02] or amoxicillin [J01CA04] or benzathine penicillin G [J01CE08] and the total number of prescriptions of systemic antibiotics [J01] associated with ICPC code R72 multiplied by 100; percentage of first-line antibiotic prescriptions associated with ICPC codes R74-R76 applying the same formula).
Data collection
We used the primary care electronic health record system of Aragon (OMI-AP), in which the diagnoses assigned to each care episode are coded applying the ICPC-28; the Pharmacy Records System (DATA de Farmacia), which includes all active electronic prescriptions funded by the Department of Health of Aragón (Servicio Aragonés de Salud, SALUD) and the guideline for empirical antibiotherapy developed by a regional group (IRASPROA).9
Ethical considerations
Raw data were aggregated and anonymised before handling to prevent identification of patients or prescribers. The study was approved by the Clinical Research Ethics Committee of Aragón (CEICA) during meeting no. 07/2020 of 01/04/2020.
Statistical analysis
We calculated the mean and standard deviation (SD) to summarise quantitative data, and absolute frequencies and percentages to summarise qualitative data. We compared qualitative data by means of the χ2 test if the data met the required conditions and otherwise using the Fisher exact test or the linear-by-linear test. The level of significance was set at 95%, and differences corresponding to p-values of 0.05 or less were considered statistically significant. We performed the data analysis with the software SPSS version 20.0.
The study was conducted in the context of the project “Criterios clínicos, test rápido de detección de antígeno estreptocócico (RADT) y tratamiento en procesos faringoamigdalares”, selected in 2018 as one of the Programmes for the Support of Initiatives for Health Care Improvement of the Department of Health of Aragón (project 2018-0079).
RESULTS
The number of documented episodes of acute respiratory tract infection (ARTI, ICPC codes R72, R74 and R76) in children included in the Teruel health care area (mean age, 9.0 ± 2.1 years; 50.9% male) was 4357 in the pre-intervention period (May 1, 2018) compared to 4045 in the post-intervention period (May 1, 2020). The prescription of systemic antibiotics for ARTI decreased in the post-intervention period compared to the pre-intervention period (44.1% of episodes compared to 46.2%; p = 0.014), and changes between the post- and pre-intervention periods in association with ICPC codes R72 (27.6% compared to 24.6%), R74 (30.6% compared to 39.9%) and R76 (41.8% compared to 35.5%) (p = 0.000) (Table 1). We found a significant increase in the percentage of the total first-line antibiotic prescriptions associated with ICPC code R72 (84.3% [415/492] compared to 57.6% [n = 285/495]; p = 0.000) and ICPC codes R74-R76 (55.2% [713/1291] compared to 45.3% [n = 688/1518]; p = 0.000) (Table 2). When it came to ICPC code R72, there was a decrease in the prescription of amoxicillin-clavulanic acid (13.6% of episodes compared to 22.9%; p < 0.001) and azithromycin (1.0% compared to 11.3%; p < 0.001) (Table 2).
| Table 1. Episodes (by ICPC code) associated with prescription of systemic antibiotics (J01) in the study period. | |||
|---|---|---|---|
| Study period | |||
| May 2018 (pre-intervention) | May 2020 (post-intervention) | p | |
| n (%) | n (%) | ||
| Total episodes with ICPC codes R72, R74 and R76 | 4357 (-) | 4045 (-) | - |
| Total episodes with ICPC codes R72, R74 and R76 associated with systemic antibiotic prescription (J01) | 2013 (46.2%) | 1783 (44.1%) | 0.014* |
| R72R74R76 | 495 (24.6%)804 (39.9%)714 (35.5%) | 492 (27.6%)546 (30.6%)745 (41.8%) | 0.000* |
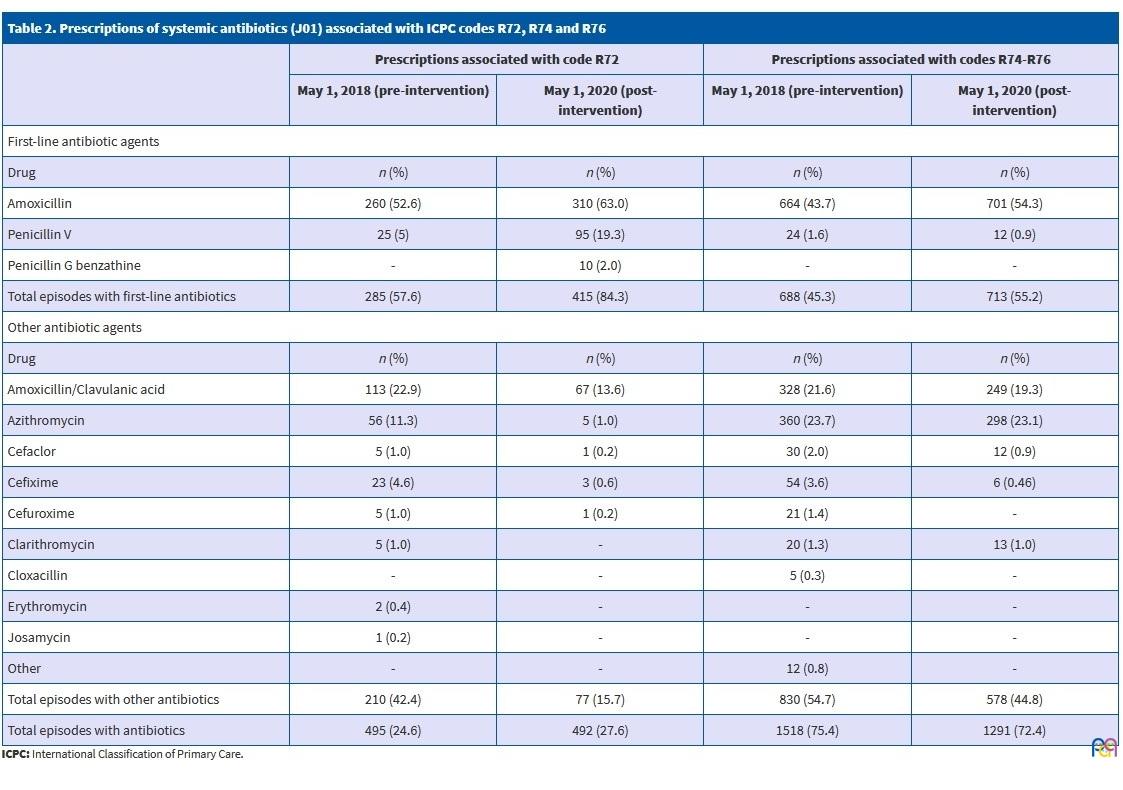
| Table 2. Prescriptions of systemic antibiotics (J01) associated with ICPC codes R72, R74 and R76 | ||||
|---|---|---|---|---|
| Prescriptions associated with code R72 | Prescriptions associated with codes R74-R76 | |||
| May 1, 2018 (pre-intervention) | May 1, 2020 (post-intervention) | May 1, 2018 (pre-intervention) | May 1, 2020 (post-intervention) | |
| First-line antibiotic agents | ||||
| Drug | n (%) | n (%) | n (%) | n (%) |
| Amoxicillin | 260 (52.6) | 310 (63.0) | 664 (43.7) | 701 (54.3) |
| Penicillin V | 25 (5) | 95 (19.3) | 24 (1.6) | 12 (0.9) |
| Penicillin G benzathine | - | 10 (2.0) | - | - |
| Total episodes with first-line antibiotics | 285 (57.6) | 415 (84.3) | 688 (45.3) | 713 (55.2) |
| Other antibiotic agents | ||||
| Drug | n (%) | n (%) | n (%) | n (%) |
| Amoxicillin/Clavulanic acid | 113 (22.9) | 67 (13.6) | 328 (21.6) | 249 (19.3) |
| Azithromycin | 56 (11.3) | 5 (1.0) | 360 (23.7) | 298 (23.1) |
| Cefaclor | 5 (1.0) | 1 (0.2) | 30 (2.0) | 12 (0.9) |
| Cefixime | 23 (4.6) | 3 (0.6) | 54 (3.6) | 6 (0.46) |
| Cefuroxime | 5 (1.0) | 1 (0.2) | 21 (1.4) | - |
| Clarithromycin | 5 (1.0) | - | 20 (1.3) | 13 (1.0) |
| Cloxacillin | - | - | 5 (0.3) | - |
| Erythromycin | 2 (0.4) | - | - | - |
| Josamycin | 1 (0.2) | - | - | - |
| Other | - | - | 12 (0.8) | - |
| Total episodes with other antibiotics | 210 (42.4) | 77 (15.7) | 830 (54.7) | 578 (44.8) |
| Total episodes with antibiotics | 495 (24.6) | 492 (27.6) | 1518 (75.4) | 1291 (72.4) |
DISCUSSION
In our study, antibiotic agents were prescribed in nearly half of the paediatric episodes of AP, which suggests that their use may not have been indicated in a large percentage of children. A previous study in the paediatric population of Aragon (0-14 years) also found a frequent use of antibiotics for management of ARTIs (34% of total cases of ARTI), and antibiotics were prescribed for management of 75% of episodes of AP.10 Acute respiratory tract infections are the main reason for antibiotic prescription in the paediatric population in Spain,11 most frequently for treatment of acute upper respiratory tract infections (AURTIs) (18.2%), acute otitis media/myringitis (14.1%), streptococcal pharyngitis/tonsillitis (12.3%) and acute tonsillitis (10.3%).3 However, these diseases also account for the highest cumulative frequency of avoidable prescriptions in healthy children, as most of these infections are viral and self-limiting.12 Thus, it is clear that antibiotic agents are frequently being prescribed for conditions for which they may not be indicated. The rational use of antibiotics constitutes responsible behaviour by clinicians in the fight against antimicrobial resistance, which poses a serious threat to global public health, but education on the subject and discussing antibiotic use with parents are also important aspects to consider when it comes to reducing the inappropriate use of antibiotics. In our study, we found a significant decrease in the proportion of episodes of AP associated with antibiotic prescriptions after the pharmaceutical education intervention, although the results were not clinically significant (overall reduction of 2%). The educational activities developed to improve antibiotic use in primary care are positive interventions that are appropriate for this care setting and perceived positively by prescribers.10 Still, there are multiple factors involved in antibiotic prescription and it is difficult to determine the one that may be most important and should be addressed by interventions to achieve the best possible outcomes. It stands to reason that antibiotic prescription would decrease and the diagnosis of R72 improve with the use of the RADT, since clinical manifestations are not sufficient to discriminate between viral and bacterial illnesses and only rapid tests have succeeded in decreasing antibiotic prescription, 6,10 but we were not able to determine the frequency of use of RADT due to gaps in the documentation of RADTs in the OMI-AP health record database and the correlation between the rapid test and the diagnosis of R72. However, improving the quality of antibiotherapy is as important as reducing its prescription when it is not indicated. As observed in other case series,10,11 we found frequent prescription of broad-spectrum antibiotics, which means that the selection of the antibiotic agent may have been inappropriate in a high percentage of patients. After the educational intervention, we found an increase in the prescription of first-line antibiotics relative to antibiotics that were not indicated. The main achievement of our study may have been the improvement in the quality of prescriptions associated with ICPC code R72, the diagnosis for which antibiotherapy is most strongly indicated, in which the proportion of prescriptions of first-line antibiotics increased from 57.6% to 84.3% of the total, with a substantial decrease in the prescription of broad-spectrum antibiotics. Inappropriate prescriptions of amoxicillin-clavulanic acid and azithromycin for management of ASP decreased significantly after the intervention, which could be due to the training received and an improved understanding of empirical treatment better suited for the specific diagnosis. When it comes to paediatric ASP, the IRASPROA guideline9 recommends azithromycin as an alternative for patients allergic to beta-lactam agents. However, we were unable to determine whether prescriptions of azithromycin in the sample had to do with risk factors in the patient, such as allergy to a certain group of antibiotics. In Aragon, a new pharmacy record system has been in use since 2016 (DATA Farmacia) based on electronic prescription and that allows linking prescriptions with the established diagnoses. This new computational tool has allowed the development and monitoring of antibiotherapy quality indicators, allowing evaluation of rational antibiotic use in relation to specific diagnoses and identification of problems in antibiotic stewardship.13 The system includes a tool that allows PC family physicians and paediatricians to check the prescriptions of specific antibiotics in all patients in their caseloads to consider the possibility of discontinuing any treatment considered inappropriate.
When it comes to the limitations of the study, we ought to highlight that while Based on the most recent data collected in the context of the PRAN, at the community level (official prescriptions within the national public healthcare system and prescriptions from private providers and insurers), in Spain there has been a 7.4% decrease in antibiotic consumption (1.9 defined daily doses per 1000 inhabitants per day [DID], with dispensation of 3 million fewer units) between 2015 and 2018, a substantial improvement considering that 93% of antibiotic consumption for human health occurs at the outpatient level.14 A systematic review (2018) found that educational interventions targeting providers and patients are associated with improved antibiotic use.15 In our study, the pharmaceutical education intervention for clinicians succeeded in reducing inappropriate antibiotic prescription for management of paediatric AP and improving the quality of antibiotic treatment. P. Lalana-Josa et al10 also concluded that an educational intervention that targeted PC paediatricians achieved an improvement in antibiotic prescription in these providers, with a reduction in prescription, although the observed differences were not statistically significant. In addition to the implementation of educational activities regarding antibiotic utilization, the PRAN contemplates other strategies to improve antibiotic prescription, such as the submission of data on antibiotic consumption indicators to prescribing physicians every 3 months or the introduction of tools to aid prescription.15 The Integral Programme for the Surveillance and Control of Healthcare-Related Infections and the Optimization of Antibiotic Utilization (IRASPROA) in the region of Aragon also refers to these processes for improving prescription in their guidelines for antibiotic treatment in PC,9 in which the setup of a consultation system in each facility is the cornerstone of the antibiotic optimization strategy. To this end, primary care scientific societies such as the Sociedad Española de Medicina de Familia y Comunitaria (semFYC) have developed educational documents for physicians and patients16 with a “DO NOT DO” approach.
Although ASP is rare in children aged less than 2 years, we included all children aged 0 to 14 years because it is the population assigned to paediatrics caseloads. In future studies, since the determinants of antibiotic prescription are very complex, it would be more useful to do a multiple intervention design to target both providers and the general population. For instance, one possibility would be to develop educational workshops for parents or infographics to teach the appropriate approach to fever and sore throat in children.
CONCLUSIONS
The pharmaceutical education intervention achieved a reduction in antibiotic prescription by PC paediatricians and optimization of the use of first-line antibiotic agents for management of the most common infectious diseases in childhood.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare in relation to the preparation and publication of this article.
ABBREVIATIONS
AC: autonomous community · AP: acute pharyngitis Primaria · ARTI: acute respiratory tract infection · ASP: acute streptococcal pharyngitis · ATC: Anatomical Therapeutic Chemical · AURTI: acute upper respiratory tract infection · CEICA: Clinical Research Ethics Committee of Aragon · ICPC: International Classification of Primary Care · PC: primary care · PCT: primary care team · PCPD: Primary Care Pharmacy Department · PRAN: National Strategy on Antimicrobial Resistances · RADT: rapid antigen detection test · SALUD: Health Department of Aragon · SD: standard deviation · UCC: urgent care centre.
REFERENCES
- Plan Estratégico y de Acción para Reducir el Riesgo de Selección y Diseminación de Resistencias a los Antibióticos (PRAN). In: Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) [online] [accessed 14/06/2021]. Available at: www.resistenciaantibioticos.es/es/profesionales/vigilancia/
- Dyar OJ, Beović B, Vlahović-Palčevski V, Verheij T, Pulcini C. How can we improve antibiotic prescribing in primary care? Expert Rev Anti Infect Ther. 2016;14:403-13.
- Base de Datos Clínicos de Atención Primaria (BDCAP). In: Ministerio de Sanidad [online] [accessed 14/06/2021]. Available at: www.mscbs.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/home.htm
- Becedo Sanz A, Cortés Rico O, García Vera C, Montón Álvarez JL. Normas de Calidad para el diagnóstico y tratamiento de la Faringoamigdalitis aguda en Pediatría de Atención Primaria. In: Protocolos del GVR (publicación P-GVR-10) [online] [accessed 14/06/2021]. Available at: www.aepap.org/gvr/protocolos.htm
- Burgaya Subirana S, Cabral Salvadores M, Bonet Esteve AM, Macià Rieradevall E, Ramos Calvo AM. Uso del test rápido de detección de antígeno estreptocócico en la consulta de Atención Primaria. Rev Pediatr Aten Primaria. 2017;19:119-25.
- García Vera C, Cemeli Cano M, Peralta Rufas EM, Romeo Lázaro E, Pina Gadea MB. Test rápido de detección de antígeno estreptocócico en faringoamigdalitis: impacto sobre el uso de antibióticos. Rev Pediatr Aten Primaria. 2017;19:345-54.
- Grupo de trabajo de Enfermedades Infecciosas de la semFYC. Manual de Enfermedades Infecciosas en Atención Primaria. 4th edition. Sociedad Española de Medicina de Familia y Comunitaria; 2017.
- WONCA International Classification Committee. Clasificación Internacional de la Atención Primaria segunda edición. ICPC-2. Barcelona: Masson; 1999.
- PROA-AP Working Group. Recomendaciones de tratamiento antibiótico empírico. In: Estrategia IRASPROA-Aragón [online] [accessed 14/06/2021]. Available at: www.aragon.es/Estrategia_irasproa/AreasTematicas/02_PROAap
- Lalana Josa P, Laclaustra Mendizábal B, Aza Pascual Salcedo MM, Carcas de Benavides C, Lallana Álvarez MJ, Pina Gadea MB. ¿Mejora la prescripción antibiótica en pediatras tras una intervención multidisciplinar? Enferm Infecc Microbiol Clin. 2015;33:78-83.
- Malo S, Bjerrum L, Feja C, Lallana MJ, Poncel A, Rabanaque MJ. Antibiotic prescribing in acute respiratory tract infections in general practice. An Pediatr (Barc). 2015;82:412-6.
- Guilliford MC, Dregan A, Moore MV, Ashworth M, Staa TV, McCann G, et al. Continued high rates of antibiotic prescribing to adults with respiratory tract infection: survey of 568 UK general practices. BMJ Open. 2014;4:e006245.
- Nota informativa 12/2019. España reduce un 7.2% el consumo de antibióticos en salud humana y un 32.4% las ventas de antibióticos veterinarios. 12 de julio de 2019. In: Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) [online] [accessed 14/06/2021]. Available at: www.aemps.gob.es/informa/notasInformativas/laAEMPS/2019/NI-AEMPS-12-2019-consumo-total-antibioticos.htm
- McDonagh MS, Peterson K, Winthrop K, Cantor A, Lazur BH, Buckley DI. Interventions to reduce inappropriate prescribing of antibiotics for acute respiratory tract infections: summary and update of a systematic review. J Int Med Res. 2018;46:3337-57.
- Recomendaciones sobre prescripción antimicrobiana en AP (Adultos). In: Agencia Española de Medicamentos y Productos Sanitarios (AEMPS) [online] [accessed 14/06/2021]. Available at: http://resistenciaantibioticos.es/es/system/files/field/files/recomendaciones_prescripcion_antimicrobiana_en_ap_adultos.pdf?file=1&type=node&id=371&force=0
- Decálogo para el uso prudente/consumo responsable de antibióticos. In: Sociedad Española de Medicina de Familia y Comunitaria (semFYC) [online] [accessed 14/06/2021]. Available at: www.semfyc.es/biblioteca/consejos-para-el-uso-prudente-de-los-antibioticos/
Comments
This article has no comments yet.