


Causes of tooth extraction
David Enrique Villares Lópeza, Antonio José Rodríguez Carravillab, Carolina Ruiz Duquec, Martín Romero Marotod
aGrado de Odontología. Universidad Rey Juan Carlos. Madrid. España .
bAlumno de Odontología. Universidad Rey Juan Carlos. Madrid. España.
cProfesora. Universidad Rey Juan Carlos. Madrid. España.
dProfesor. Universidad Rey Juan Carlos. Madrid. España.
Correspondence: DE Villares. E-mail: davide.villareslopez@gmail.com
Reference of this article: Villares López DE, Rodríguez Carravilla AJ, Ruiz Duque C, Romero Maroto M. Causes of tooth extraction. Rev Pediatr Aten Primaria. 2016;70:e73-e79.
Published in Internet: 28-04-2016 - Visits: 13079
Abstract
Introduction: to know the causes of tooth extraction in child population, both deciduous and definitive dentition, is necessary to be able to appreciate the impact of the preventive measures, as well as determine the intervention in matters of oral health to get a healthy population.
Materials and methodologies: epidemiologic, observational, descriptive and transversal study is designed in the usual practice of odontology. Its population consisted of people under the age of 18 who went to University clinic, and those who got one or more teeth extracted.
Results: 97 removals were made to 55 patients (4% of treated population), 58.8% were female patients. The average age was 8.69 (EV 2.15). The most frequent age range to have teeth extracted was from 6 to 10 years old (52.6%). Dental growing disorder was the most frequent cause of tooth extraction (39.2%), followed by caries (34%). In inmigrant population the most frequent cause was the caries (69.76%).
Conclusions: it is necessary to introduce, from pediatric consulting rooms in odontology, preventive measures in the population from 6 to 10 years old, reinforcing dietary and nutritional habits which facilitate a proper reabsorption of deciduous dentition, to decrease the number of extractions and to get a good oral health.
Keywords
● Children ● Oral health ● Removal ● Tooth extractionINTRODUCTION
Tooth extraction is one of the commonly performed procedures in the university clinic. The aim of this study was to assess the reasons for tooth extraction, both of primary and permanent teeth, in the paediatric population.
Having knowledge of these causes will allow us to act, implementing health promotion and disease prevention strategies to reduce the number of tooth extractions performed in the paediatric population and contributing to an overall improvement in their oral and dental health.
In Spain, the 2010 Oral Health Survey1 reported a frequency of tooth extractions that ranged between 2.2% and 3.5% in cohorts of children aged 12 to 15 years and the reasons for these interventions, but more specific studies are required to better describe the current situation of orodental health in the paediatric population.
At present, tooth extraction is one of the surgical procedures performed most frequently in dental clinics in Spain, with a frequency of 37% to 66%, and accounting for nearly 90% of all surgical procedures in this setting.2-4
The General Board of Dentists of Spain (Consejo General de Colegios de Odontólogos y Estomatólogos de España) has established that the main indications for tooth extraction are: severe decay in a tooth that cannot be restored or rehabilitated; abnormalities in tooth location or position that cause other abnormalities that cannot be resolved with another approach, and orthodontic, prosthetic or surgical reasons.5
Currently, numerous studies are focusing on the reasons why tooth extraction is used in the adult population, but there is very little information on this subject for the paediatric population, which is what makes this study pertinent and relevant.
The core of the work in a dental clinic is to implement health promotion and disease prevention strategies with the purpose of increasing the quality of life of patients, and thus, these two factors are key in the paediatric population.
Therefore, it is important to launch interventions to promote dental hygiene, as this is a key priority, along with nutritional counselling, which could include recommendations and directions regarding food selection and dietary habits to help prevent caries and periodontal disease, or to promote the development of jawbones and thus favour tooth replacement. These interventions are more effective if they are implemented with the cooperation of health providers involved in paediatric health, so communication and coordination among all, including paediatricians, family physicians, nurses, dental hygienists and dentists, is of the essence.
For this reason, we proposed the performance of a study in the Universidad Rey Juan Carlos (Madrid, Spain) to analyse the reasons leading to tooth extraction in the paediatric population, converging with one of the orodental health goals in Spain for year 2020,6 which is to advance health promotion and prevention strategies, especially in children and youth. We also sought to analyse the distribution of tooth extractions by age, sex, nationality, number of teeth extracted and reasons for the extraction, and to determine which teeth are most likely to be extracted.
MATERIALS AND METHODS
We conducted an epidemiological, observational, descriptive, cross-sectional field study of everyday clinical practice in the context of the practicum of the course on Integrative Paediatric Clinical Dentistry carried out at the University Clinic of the Universidad Rey Juan Carlos (URJC).
The population under study consisted of the patients aged less than 18 years that sought services at the clinic either on their own initiative or following referral by a different health care provider between October 2014 and February 2015, in whom tooth extraction was recommended following an orodental evaluation, and that consented to the collection of data for the purposes of this study.
The sample was obtained by consecutive selection of patients that met the previously mentioned inclusion criteria, excluding patients that refused to participate.
We documented all the tooth extractions performed during this period, collecting data for the variables that follow:
- Dependent variable. Cause of tooth extraction: categorical variable with seven categories: 1) dental caries: conservative treatment was not indicated or had failed; 2) periodontal disease: advanced periodontal disease with marked tooth mobility and presence of periodontal abscesses precluding conservative surgical treatment is a frequent indication for tooth extraction; 3) mixed: dental caries + periodontal disease; 4) trauma (acute or chronic): a tooth can be preserved as long as it is not infected and does not interfere with correct occlusion; 5) orthodontic indications; 6) abnormalities in tooth eruption, including teeth with abnormal exfoliation that impede or alter the eruption of permanent teeth, and 7) other causes not included in the previous sections: prostheses, attrition, malposition or impaction.
- Independent variables: 1) age: continuous quantitative variable; 2) sex: dichotomous variable (male/female); 3) number of tooth extractions per patient: discrete quantitative variable; 4) type of tooth extraction: dichotomous categorical variable (single/multiple); 5) extracted tooth, using the FDI World Dental Federation notation: categorical variable with 32 categories7; and 6) origin: country of birth, dichotomous categorical variable (Spanish/immigrant).
The diagnosis and treatment of the patients included in the study were performed by the two authors of this article. In all patients, after students performed the examination and made a diagnosis, and under the guidance of the faculty, it was decided whether one or more tooth should be extracted, adhering to the criteria for tooth extraction established by The General Board of Dentists of Spain,5 and specifying the reasons for the procedure.
We recorded the data and subsequently analysed them using the SPSS® 19.0 software. We calculated the mean and standard deviation for quantitative variables, and frequencies and percentages for categorical variables.
We requested the informed consent of the patients for their participation in the study, which was granted by a parent or legal guardian. The confidentiality of patients was guaranteed, as the study did not require any personally identifiable information.
RESULTS
During the period under study, a total of 1373 patients received care in the University Clinic of the URJC, with a mean daily caseload of 31.07 patients.
Of the 1373 patients, 55 (4%) underwent tooth extractions. All extractions involved primary teeth, and none were extractions of permanent teeth.
The mean age of patients that underwent tooth extraction was 8.69 years (standard deviation [SD], 2.15); 20 were male (36.4%) and 35 female (63.6%); 43 were of Spanish descent (78.2%) and 12 immigrants (21.8%), with the latter originating most frequently from Pakistan (5.5%), followed by China (3.6%).
A total of 97 extractions were performed, of which 40 were done in male patients (41.2%) and 57 in female patients (58.8%). Seventy-four extractions (76.3%) were performed in patients of Spanish descent and twenty-three (23.7%) in immigrant patients. Single tooth extractions were performed in 29 patients, and multiple tooth extractions in 26, with a mean of 2.61 teeth removed in each multiple procedure.
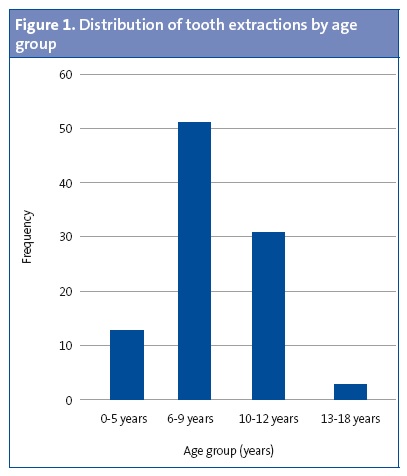
Figure 1 shows the frequency of tooth extractions by age group. The age group in which tooth extractions were performed most frequently was children aged 6 to 10 years (52.6%), followed by children aged 10 to 13 years (32%).
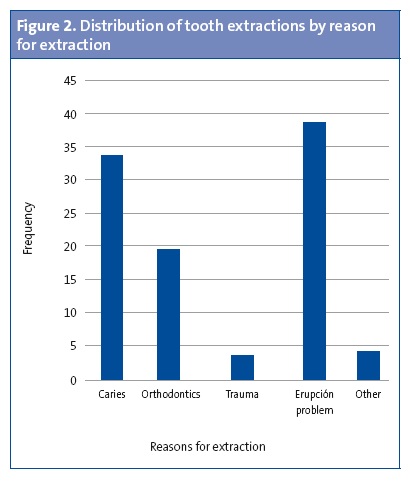
The most frequent indication for tooth extraction was tooth eruption problems, which gave rise to 38 extractions (39.2%), of which 93% were due to abnormal reabsorption of the primary tooth, and 3% of these to the presence of ectopic molars (Figure 2). Extractions due to dental caries amounted to 34% of the total, extractions related to orthodontics to 19.6%, extractions due to trauma to 3.1%, and extractions due to other reasons to 4.1% (internal tooth resorption in 1.03% and cleft-palate in 3.09%).
The mean age at which teeth were extracted due to problems with tooth eruption was 9.07 years, while the mean for teeth extracted due to caries was 7.21 years, and for the purposes of orthodontics, 9.68 years.
Our analysis by sex showed that 47.5% of tooth extractions in male patients were due to tooth eruption problems, 40% to dental caries, and 7% for orthodontic reasons. In female patients, problems in tooth eruption accounted for 33.3% of extractions, caries for 29.8%, and orthodontics for 28.07%.
The distribution of the reasons for tooth extraction in the group of patients that were Spanish nationals differed from the distribution in the immigrant group, a difference that was statistically significant (P < .0001). In Spanish patients, problems with eruption accounted for 47.29% of extractions, and caries and orthodontics for 22.97%. In immigrant patients, the most frequent reason for tooth extraction was dental caries (69.56%), while tooth eruption problems were not as frequent (13.4%), and only 8.69% of extractions were done for the purposes of orthodontics.
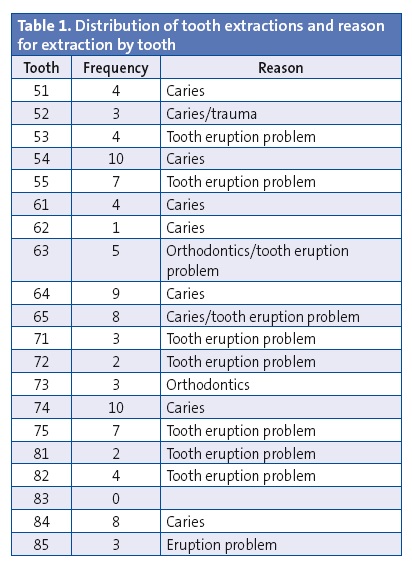
Extractions of posterior teeth (63.9%) were more frequent than extractions of anterior teeth (36.1%), with caries being the most frequent reason for extraction of posterior teeth (41.93%), followed by eruption problems (37.09%). For anterior teeth, the most frequent reason for extraction was tooth eruption problems (42.85%), followed by caries and reasons related to orthodontics, both of which accounted for 20%. All extractions due to trauma were of anterior teeth, and extractions due to trauma accounted for 8.57% of the total extractions performed (Table 1).
DISCUSSION
When comparing different studies, it is important to take into account their methodology, the population under study and the inclusion criteria, as variability in these aspects could invalidate comparisons. For this reason, we have restricted the discussion of our research to specific aspects.
The only studies we found that analysed the causes of tooth extractions in paediatric samples were those conducted by Alsheneifi and Hughes,8 and by Lucavechi, Suárez and Barbería.9 However, our study differs in that we conducted our research following diagnosis in the context of face-to-face clinical visits, as opposed to by retrospective review of clinical records.
Our study found that the mean age of patients that underwent teeth extractions (4%) was 8.69 years (SD, ± 2.15). The age group in which extractions were performed most frequently was the 6-to-10 year group (52.6%), followed by the 10-to-13 years group (32%). In the study by Lucavechi-Alcayaga,9 the mean age of patients was 7.76 years (SD, ± 2.91). As happened in our study, the age group in which extractions were performed most frequently was the 6-to-10 years group (45.01%).
The difference between sexes in the absolute frequency of tooth extractions (41.2% in boys and 58.8% in girls) was not statistically significant, which was consistent with the findings of other studies.8,9
As for the type of extractions performed, in our study we observed that multiple extractions were performed in 47.3% of patients, compared to 53% in the study by Alsheneifi8 and 68.33% in the study by Lucavechi-Alcayaga.9.
When we analysed the reasons for tooth extraction in our study, we found that the most frequent reason was abnormal tooth eruption (39.2%), compared to dental caries in the study by Alsheneifi8 (53%), and orthodontics-related reasons in the study of Lucavechi-Alcayaga9 (44.75%). This difference may be due to the particular characteristics of each facility: the study by Alsheneifi8 was conducted in a hospital clinic, while the study by Lucavechi-Alcayaga9 was conducted in a university clinic that offered integral care, including care for paediatric dental diseases and orthodontics.
Caries was the second most frequent reason for tooth extraction in our study (34%), and orthodontic-related reasons were third (19.6%) and peaked between ages 6 and 12 years, which we expected since these are the ages at which orthodontic treatments are performed most often. When we reviewed the scientific literature, we found that the leading reason for extractions in patients aged less than 16 years is orthodontics.5,8,10-13
When it came to the distribution of reasons for extraction in the Spanish and immigrant patients, we found statistically significant correlations. However, we did not find any studies analysing this factor. This substantial difference could be attributed to social and health differences that lead to better or worse hygiene and orodental care related to access barriers in private dental care.
When we analysed the reasons for tooth extraction by sex, we found that the most frequent reason for extraction in male patients was eruption problems (47.5%), which was the case in female patients (33.3%). However, a higher proportion of extractions related to orthodontics were performed in female patients (84.21%) that in male patients (15.78%). This is consistent with the results obtained by Hull.12
Most extractions involved posterior teeth, consistent with the findings of most previous studies.8,9,14 The teeth extracted most frequently in our study were teeth 54 and 74, and the most frequent indication for the extraction of both of these teeth was caries, which was consistent with the data reported by Alsheneifi8 and Lucavechi-Alcayaga.9
CONCLUSIONS
- Problems with tooth eruption due to abnormalities in the reabsorption of primary teeth were the most frequent cause of tooth extraction. This calls for the implementation of preventive measures in the 6-to-10-year-old population to promote dietary and nutritional habits that would facilitate the correct reabsorption of primary teeth, which has been affected in recent years by the popularity of softer foods (sandwich bread, baked goods…).
- Since caries was the most frequent reason for tooth extraction in the immigrant population, interventions in this population should consist of preventive measures to promote hygiene and good dietary habits.
- The primary first molars were the teeth extracted most frequently, so it is important that preventive programmes are implemented to promote oral hygiene habits, including correct tooth brushing technique, with emphasis on these teeth.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.
ABBREVIATIONS: SD: standard deviation · URJC: Universidad Rey Juan Carlos.
REFERENCES
- Llodra Calvo JC. Encuesta de salud oral en España 2010. Análisis de la evolución de la salud oral de 1993 a 2010. RCOE. 2012;17:13-41.
- Varela Centelles PI. Evolución de la demanda odontológica en la Atención Primaria reformada. Cuadernos de Atención Primaria. 2001;8:259-64.
- Tapias Ledesma MA. Características de la consulta a demanda de una unidad de salud bucodental en un Centro de Salud de Móstoles. Arch Odontoestomatol. 2005;21:160-6.
- Donado M. Cirugía bucal. Patología y técnica. 3.ª edición. Barcelona: Masson; 2005. p. 298-304.
- Ilustre Consejo General de Colegios de Odontólogos y Estomatólogos de España. Código de tratamientos, actos dentales y nomenclator. In: Colegio Oficial de Dentistas de Bizkaia [online] [consulted on 21/03/2016]. Available in www.coeb.com/wp-content/uploads/2014/04/glosario.pdf
- Llodra Calvo JC, Bourgeois D. Estudio prospectivo Delphi. La salud bucodental en España 2020. Tendencias y objetivos de salud oral. In: Consejo General de Odontólogos y Estomatólogos de España [online] [consulted on 21/03/2016]. Available in www.consejodentistas.es/pdf/0912%20Libro%20Estudio%20Delphi.pdf
- Keyserr-Neilsen S. FDI two digits system of the designating teeth. J Dent. 1971;21:104-6.
- Alsheneifi T, Hughes C. Reasons for dental extractions in children. Pediatr Dent. 2001;23:109-12.
- Lucavechi-Alcayaga T, Suárez-Clúa MC, Barbería-Leache E. Estudio de la prevalencia y causas de las exodoncias en una población infantil española. RCOE. 2004;9:65-72.
- Ong G, Yeo J, Bhole S. A survey of reasons for extraction of permanent teeth in Singapore. Community Dent Oral Epidemiol. 1996;24:124-7.
- McCaull L, Jenkins W, Kay E. The reasons for the extraction of various tooth types in Scotland: a 15 year follow up. J Dent. 2001;29:401-7.
- Hull PS, Worthington HV, Clerehugh V, Tsirba R, Davies M, Clarkson JE. The reason for tooth extractions in adults and their validation. J Dent. 1997;25:233-7.
- Cahen PM, Frank RM, Turlot JC. A survey of the reasons for dental extractions in France. J Dent Res. 1985;64:1087-93.
- Villares López DE, Rosado Olarán JI, Villares Rodríguez JE, González González AI, Rodríguez Barrientos R. Análisis de las causas de exodoncia en dentición permanente en pacientes que acuden a la consulta de odontología de un centro de salud de Atención Primaria. Cient Dent. 2015;12:7-14.
Comments
This article has no comments yet.