

Vol. 23 - Num. 92
Original Papers
Survey on the approach to diagnosis and rational use of antibiotics in paediatric respiratory illness in Primary Care
Verónica Fernández Romeroa, M.ª Elena Cabezas Tapiab
aPediatra. CS Vélez Málaga-Sur. Vélez-Málaga. Málaga. España.
bPediatra. CS de Villaviciosa de Odón. Villaviciosa de Odón. Madrid. España.
Correspondence: V Fernández. E-mail: veronicafernandez565@gmail.com
Reference of this article: Fernández Romero V, Cabezas Tapia ME. Survey on the approach to diagnosis and rational use of antibiotics in paediatric respiratory illness in Primary Care. Rev Pediatr Aten Primaria. 2021;23:353-64.
Published in Internet: 12-11-2021 - Visits: 7328
Abstract
Introduction: respiratory infections are the most frequent presenting complaint and reason for prescription of antibiotherapy in paediatric care. Antibiotic resistance is a public health problem. Objective: to assess antibiotic prescription practices in the management of paediatric respiratory illness throughout Spain.
Material and methods: we conducted a survey of Spanish paediatricians distributing a questionnaire by email. The statistical analysis was performed with the software SPSS version 20.0.
Results: we received 362 responses. We found that 53.1% of respondents managed 25-35 patients daily. The mean number of correct answers was 18.8 out of 23. In the case of acute otitis media, respondents determined the indication and duration of antibiotherapy based on different criteria and in variable percentages; 98.6% used amoxicillin, and 97.2% prescribed it at correct doses. In the case of pharyngitis, 79.1% ordered microbiological tests, 50.8% prescribed amoxicillin and 48.6% penicillin, and 84% prescribed treatment for 10 days. When it came to respiratory illnesses of viral aetiology (bronchospasm, common cold and bronchiolitis), more than 90% did not prescribe antibiotics, although the presence of high fever or green nasal discharge was associated with more frequent prescription. In the case of typical pneumonia, up to 59.6% did not order a chest radiograph, 94.1% prescribed amoxicillin, and 68.3% prescribed treatment courses lasting 7 days. For atypical pneumonia, 97.8% prescribed macrolides. We found a statistically significant association between the years of experience and both the score in the questionnaire and the use of chest radiography; between the speciality of the clinician and the questionnaire score, and between physician workload and the ordering of microbiological tests in cases of pharyngitis.
Conclusions: we found mistakes in the use of antibiotherapy in paediatric care. Strategies need to be developed to educate the population and health care providers to promote the rational use of antibiotics.
Keywords
● Antibiotics ● Appropriate prescribing ● Paediatrics ● Respiratory tract infectionINTRODUCTION
Respiratory infections are the main reason for paediatric primary care visits1-3 and the most frequent reason for antibiotic prescription. Deciding whether an antimicrobial is necessary, when to initiate such treatment and how to select the most appropriate agent, prescribing it at the correct dose and for the correct duration, is a challenge in clinical practice.
Spain is one of the countries with the highest unwarranted consumption of antibiotics in humans and one of the countries in Europe with the highest rates of antimicrobial resistance, and infections by drug-resistant pathogens has become an important public health problem.4-6
One of the main factors that promote the development and spread of multidrug-resistant bacteria is the irrational use of antibiotics. According to the SEIMC-SEFH-SEMPSPH consensus document on bacterial drug resistance, the education of health care workers and the general population on the prevention, diagnosis and treatment of infectious diseases is deficient in Spain, which explains the heterogeneity in their management and the increase in antimicrobial resistance. 4-6
The aim of our study was to describe antibiotic prescription practices in the management of paediatric respiratory infections at the primary care level and to assess the association of these practices with the years of experience, urban vs. rural setting, medical speciality (paediatrician vs. other) and workload. We also assessed whether, in the context of a given disease, the presence of high fever or greenish secretions was associated with a greater likelihood of antibiotic prescription. The ultimate purpose of the study was to acquire knowledge to guide the development of effective strategies to promote the rational use of antibiotics.
MATERIAL AND METHODS
We conducted an observational, descriptive and analytical study. We designed an anonymous semi-structured questionnaire with 33 items: 4 on the characteristics of the provider and the work setting; 1 on the workload of the physician; 16 direct questions on the clinical criteria for indication of antibiotherapy, the selection of the antibiotic agent, its dose and duration; 2 on the performance of diagnostic tests (microbiological tests in pharyngotonsillitis and plain radiograph of the chest in pneumonia); 7 on hypothetical cases of children with complaints commonly found in paediatric practice but with no diagnosis given; 3 on the attitudes and influence of parents or caregivers in prescription; and 2 on the factors that the respondent believed contributed most to the irrational use of antibiotics.
We assessed the appropriateness of prescription based on the current scientific evidence available for Spain, based on: The empirical antibiotherapy guideline (Guía ABE), the diagnostic and therapeutic protocols of the Asociación Española de Pediatría (Spanish Association of Pediatrics, AEP), the algorithms of the Asociación Española de Pediatría de Atención Primaria (Spanish Association of Primary Care Paediatrics, AEPap) and consensus documents published in Spain.4-23
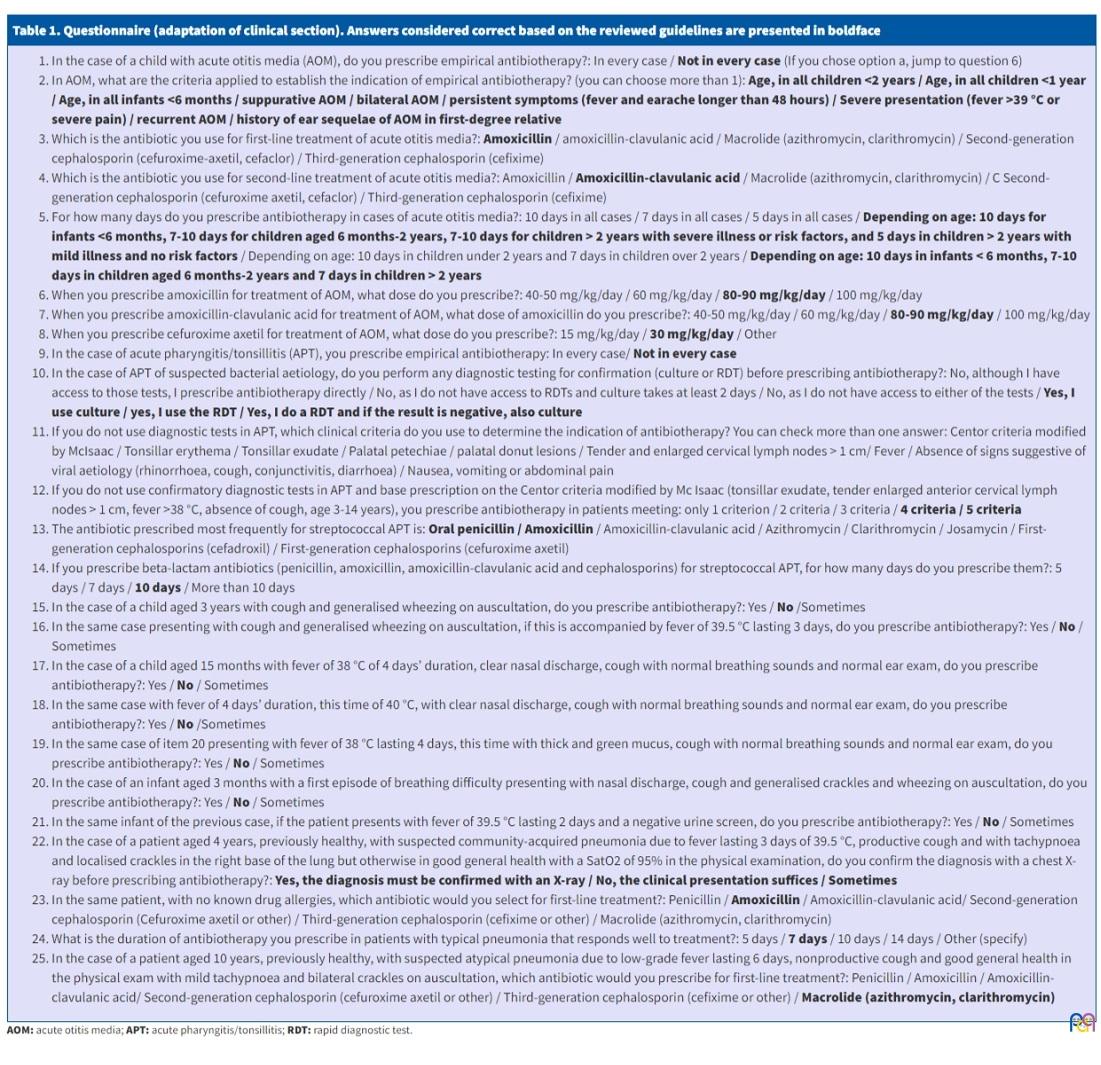
Table 1 presents an adaptation of the questionnaire that shows the clinical sections with the answer choices, with the answers considered correct shaded.
| Table 1. Questionnaire (adaptation of clinical section). Answers considered correct based on the reviewed guidelines are presented in boldface |
|---|
|
The questionnaire was distributed by email to physicians in Spain employed in paediatric care through the mailing list of the PEDIAP and by submitting each of the regional associations affiliated to the AEPap to distribute the email to their members. We chose these channels because it would allow us to reach the largest possible number of professionals practicing primary care paediatrics.
We created a Microsoft Excel spreadsheet to enter the data. The statistical analysis was performed with the software SPSS 20.0 for Windows. We analysed the association between the results of the survey and the following variables: work experience (in years), medical speciality (paediatrician vs medical intern-resident [MIR] vs other education), work setting (urban vs rural vs combined) and workload (number of patients managed per day).
RESULTS
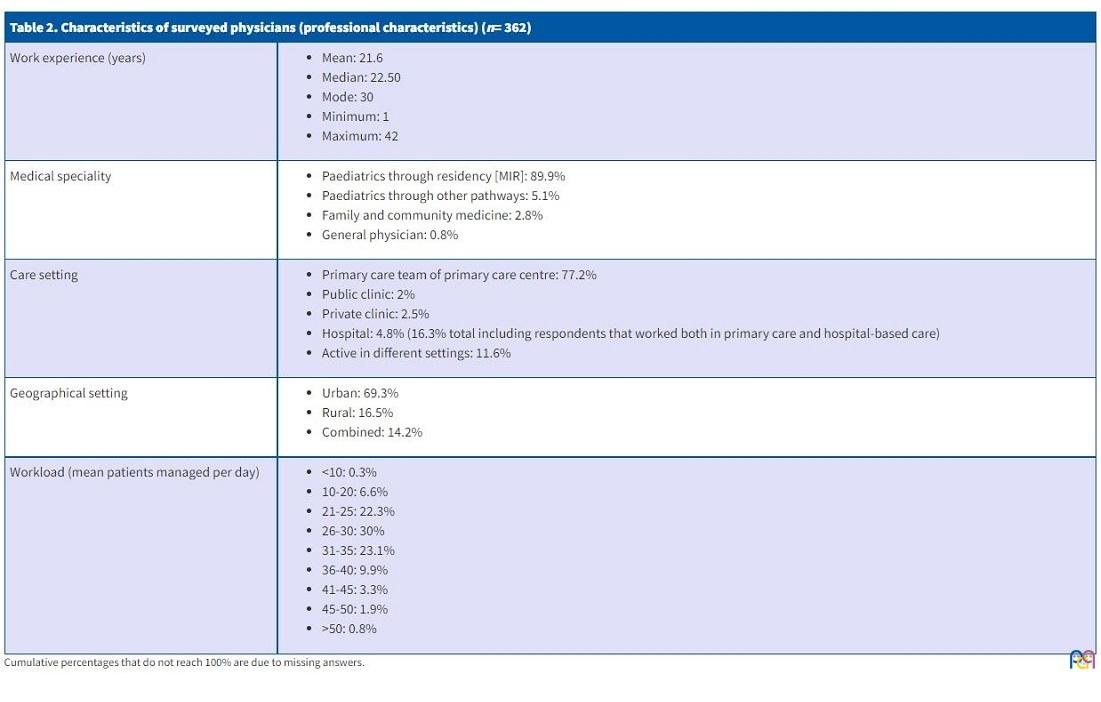
We received 362 responses to the questionnaire. Table 2 summarises the data corresponding to the education and work characteristics of the physicians. The data on the diagnosis and management of diseases by respondents is summarised in Table 3.
| Table 2. Characteristics of surveyed physicians (professional characteristics) (n = 362) | |
|---|---|
| Work experience (years) |
|
| Medical speciality |
|
| Care setting |
|
| Geographical setting |
|
| Workload (mean patients managed per day) |
|
| Table 3. Diagnostic and therapeutic practices based on participant responses (n = 362). Answers considered correct are presented in boldface |
|---|
| Management of acute otitis media:
1. Antibiotherapy in every case: Yes, 3.7%; No: 96.3% 2. Criteria for indication of antibiotherapy:
3. First-line antibiotic: Amoxicilina: 98.6%, First-line antibiotic: 1,1% 4. Second-line antibiotic:
5. Prescribed antibiotic dose
6. Duration of antibiotherapy:
|
| Management of acute pharyngitis/tonsillitis:
7. Antibiotherapy in every case: Yes, 1.4%, No, 96.4% 8. Performance of microbiological testing to detect pyogenes before prescribing antibiotherapy:
9. In the case of not performing microbiological testing, respondents applied the following criteria:
10. In case confirmatory diagnostic tests are not used in APT and prescribing is based on the Centor criteria modified by Mc Isaac (tonsillar exudate, tender enlarged anterior cervical lymph nodes > 1 cm, fever >38 °C, absence of cough, age 3-14 years), respondents prescribed antibiotherapy in patients meeting:
11. Most frequently prescribed antibiotic: Oral penicillin: 48.6%, Amoxicillin: 50.8%, Amoxicillin-clavulanic acid: 0.6%, other: 0% 12. Prescribed duration of treatment with beta-lactam antibiotic: 10 days: 84%, 7 days: 14.3%, Otra: 3.7% |
| Management of bronchospasm (clinical cases in items 20 and 21):
13. Afebrile bronchospasm, prescribes antibiotherapy: Yes, 0%; No, 96.9%, Sometimes, 2,8% 14. Bronchospasm with high fever lasting 3 days, prescribes antibiotherapy: Yes, 10.1%; No, 50.6%; Sometimes: 39.3% |
| Management of upper respiratory infection/cold (clinical cases in items 22, 23 and 24):
15. Cold symptoms with low-grade fever and clear nasal discharge, prescribes antibiotherapy: Yes, 0.6%; No, 90.4%; Sometimes, 9% 16. Cold with high fever and clear mucus, prescribes antibiotherapy: Yes, 8.1%; No, 50%; Sometimes, 41.9% 17. Cold with low-grade fever and thick and green mucus, prescribes antibiotherapy: Yes, 5.6%; No, 59%; Sometimes, 35.4% |
| Management of bronchiolitis (clinical cases in items 25 and 26):
18. Bronchiolitis in infant aged 3 months, afebrile, prescribes antibiotherapy: Yes, 2.2%; No, 94.4%; Sometimes, 3.4% 19. Bronchiolitis in infant aged 3 months with high fever, prescribes antibiotherapy: Yes, 13.2%; No, 58.3%; Sometimes, 28.5% |
| Management of typical community-acquired pneumonia (clinical case in items 27-29):
20. Orders chest x-ray to confirm diagnosis prior to antibiotic prescription in healthy child in good general health with a normal oxygen saturation: Yes: 14.9%, No: 59.6%, Sometimes: 25.6% 21. First-line antibiotic: Amoxicillin: 94.1%, Amoxicillin-clavulanic acid: 4.2%, Macrolide: 1.4%, other: 0% 22. Duration of antibiotherapy for typical pneumonia with favourable response: 7 days: 68.3%, 10 days: 30.1%, 5 days: 1.1%, 14 days: 0.6% |
| Management of atypical community-acquired pneumonia (clinical case in item 30):
23. First-line antibiotic: Macrolide (clarithromycin or azithromycin), 97.8%, Amoxicillin: 1.7%, Amoxicillin-clavulanic acid: 0.6% |
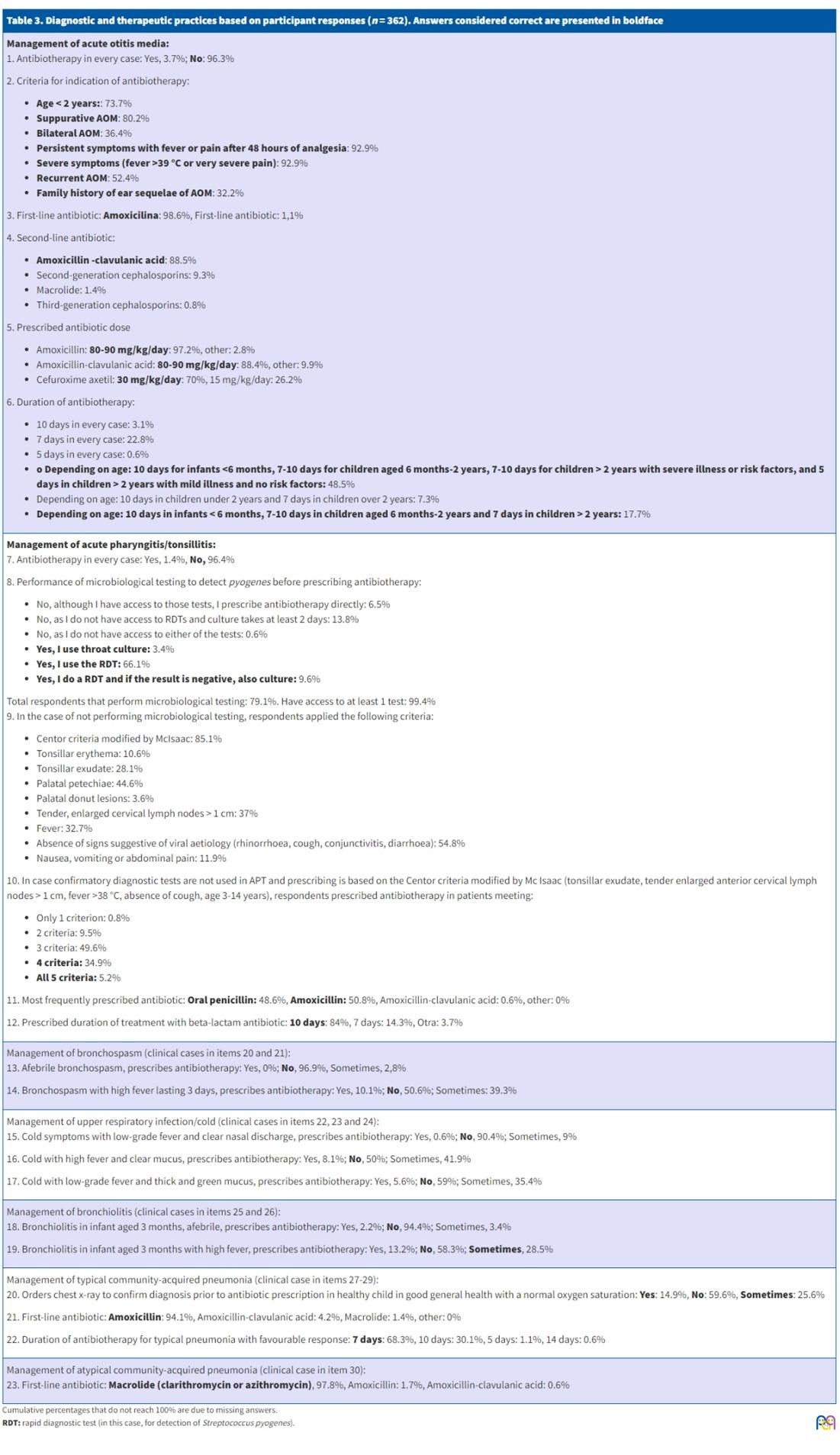
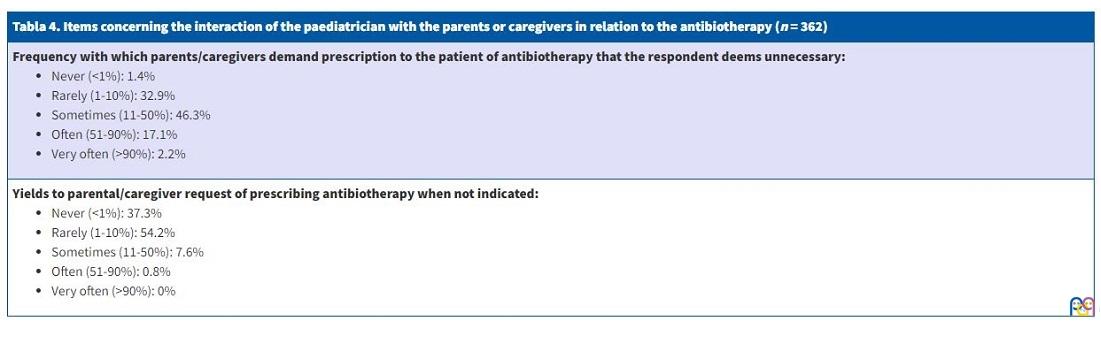
Table 4 presents the answers to items about the attitudes of parents or caregivers regarding antibiotic use and the pressure they exert on health care providers.
| Tabla 4. Items concerning the interaction of the paediatrician with the parents or caregivers in relation to the antibiotherapy (n = 362) |
|---|
Frequency with which parents/caregivers demand prescription to the patient of antibiotherapy that the respondent deems unnecessary:
|
Yields to parental/caregiver request of prescribing antibiotherapy when not indicated:
|
When asked which factor they believed had the most impact on the irrational use of antibiotics, 43.1% of respondents answered it was their workload, 18.6% parental/caregiver pressure, 16% the need to be “efficient” in care delivery (prevent new appointments or evaluations), 11.7% fear of lawsuits due to poor outcomes in some patients, and 10.6% other factors.
When asked what they believed could contribute most to reducing the irrational use of antibiotics, 39.7% of respondents answered it would be educating the population, 38.3% the availability of resources in the clinic to facilitate more accurate management of the most common illnesses (pneumatic otoscopy for diagnosis of acute otitis media [AOM], rapid streptococcus test for acute pharyngitis/tonsillitis [APT], rapid viral detection tests …), 15.2% to reduce physician workloads, 0.6% all of the above, and the rest other aspects.
We found a statistically significant negative association, albeit of small magnitude, between the work experience in years and the score in the questionnaire, meaning that providers that had more experience had lower scores. We also found a statistically significant association between the years of work experience and the performance of a chest X-ray in case of suspected typical pneumonia in healthy children: more experienced providers were less likely to order X-rays. When we compared the medical education of the provider and the score in the questionnaire, we found that physicians that had specialised in paediatrics scored higher compared to other physicians, a difference that was statistically significant. Lastly, we found a significant association between physician workload and the performance of microbiological testing for diagnosis of pharyngitis/tonsillitis before prescribing antibiotics that evinced a negative impact: physicians with heavier workloads were less likely to order confirmatory tests. We did not find any other statistically significant associations in the rest of the comparisons with the variables under study.
DISCUSSION
One of the limitations of our study was that, although we conducted a survey of nationwide scope, the response rate was of only 5.65% (362 physicians out of the total 6402 primary care paediatrics providers), which carries a risk of selection bias, as respondents had to be subscribed to mailing lists, know how to use the software tools used in the survey and be willing to participate. Physicians who were less aware of antibiotic stewardship were probably less likely to respond.24 Therefore, while our survey contributes information on current prescription trends in the group of respondents, extrapolating the results to the entire population of physicians working in primary care paediatrics in Spain would not be appropriate. We also took the responses of physicians as accurate, but there may be differences between what they have reported in the survey and their actual real-world practices.
Bacterial drug resistance is a public health problem. Resistance to different drugs emerges due to overprescription, inappropriate selection of the drug based on its profile or inappropriate dose or duration of treatment.
The following aspects need to be considered for appropriate prescription of empirical antibiotherapy:
- High probability of a bacterial aetiology given the clinical presentation and epidemiological context, supported by rapid diagnostic tests or other resources when possible.
- Knowledge of the microorganisms most frequently involved in each infection and local antimicrobial resistance trends.
- Toxicity and potential adverse effects of each of the available antibiotics.
- Facilitating adherence: convenient dosing, tolerability, optimal duration of treatment.
Based on a Cochrane review published in 2015, antibiotherapy offers limited benefits in the management of AOM in paediatric patients, with greater benefits in children under 2 years with bilateral or suppurative AOM.26 Given that more than 80% of cases resolve spontaneously, this benefit must be weighed against the potential toxicity of antimicrobials. Of all respondents, 96.3 % selected the cases of AOM for which antibiotherapy was indicated and did not prescribe it in every case. The criteria applied more frequently to determine the indication were: age less than 2 years, suppuration, severe presentation (fever > 39 °C or intense pain) and persistence of symptoms after 48 hours of prescribed analgesia. In adherence with the reviewed guidelines, most respondents selected amoxicillin for first-line treatment and amoxicillin-clavulanic acid for second-line treatment, and the correct dosage with prescription of high doses of amoxicillin (80-90 mg/kg/day) due to the prevalence of drug resistance in Streptococcus pneumoniae in Spain.4-7 The variability in the duration of antibiotherapy may be justified by differences in the indications given in different guidelines4-7 (Table 1).
The aetiology of APT is usually viral. Among bacterial pathogens, the most frequent causative agent is Streptococcus pyogenes or beta-haemolytic group A streptococcus (BHGAS), responsible for 30-40% of cases of APT in children aged 3-13 years, 5-10% of children aged 2-3 years and only 3-7% of children under 2 years.9,10 Consistent with this fact, 96% of respondents did not routinely prescribe antibiotics for management of APT.
In most cases, it is difficult to differentiate between a viral and a streptococcal aetiology in APT. The responses of physicians as to the clinical criteria they considered in their decision-making were heterogeneous. The manifestations suggestive of a streptococcal aetiology are sore throat with an abrupt onset, fever (although fever, including high-grade fever, is also frequently present in viral cases), general malaise and headache, in addition to abdominal pain, nausea and vomiting, especially in young children. The presence of palatal petechiae is not exclusively associated with APT due to BHGAS, as these lesions may also develop in viral infections, but 45% of respondents considered it indicative of a bacterial aetiology.10 The presence of what is known as “doughnut” lesions in the palate, small erythematous papules with a pale centre, is pathognomonic, as these lesions have only been described in APT due to BHGAS, but only 3.6% identified it as a discriminant of the aetiology of APT.10 The absence of signs suggestive of viral infection (rhinorrhoea, cough, conjunctivitis or diarrhoea) was a criterion selected by more than 50% of respondents. Tonsillar exudate is found frequently in viral infections (adenovirus, infectious mononucleosis), so, absent other signs and symptoms, it is not a relevant criterion for differential diagnosis, as believed by more than 70% of respondents.10 Differentiation based solely on the use of the Centor criteria modified by McIsaac is not appropriate, as streptococcus is only involved in 38-63% of APT cases with scores of 4 or 5 points, and therefore using these criteria alone can contribute to overdiagnosis and prescription of unnecessary antibiotherapy.10
Thus, given the nonspecificity of the symptoms for the purpose of establishing the aetiology of APT, it is necessary to perform microbiological tests for detection of BHGAS in carefully selected cases with signs suggesting a likely streptococcal aetiology, but not when a viral aetiology is suspected.8-11 Establishing eligibility for testing is not only necessary for economic reasons, but also because these tests cannot differentiate between active infection and carrier status.10
There are two types of diagnostic tests for detection of BHGAS: streptococcus antigen rapid detection test (RDT) and throat swab culture.8-11 Based on its high specificity, if the RDT is positive, BHGAS is accepted as the aetiological agent of APT and confirmation by culture is not necessary. However, if the results are negative, some experts recommend routine performance of culture, which offers a sensitivity of 90-95% and a specificity of 99%. The most significant drawback of culture is that results are obtained, at best, in 24 to 48 hours.10 Nearly all respondents (99.4%) had access to the RDT for Streptococcus pyogenes, but only 79% ordered them, mainly due to their heavy workloads (the heavier the workload, the less likely respondents were to order diagnostic tests for APT, probably because of the time it involves).
Antibiotherapy is indicated and warranted for management of streptococcal APT, as it achieves quicker resolution of symptoms, reduces the time the patient is contagious and prevents local suppurative and nonsuppurative complications.9,10
Penicillin is the drug of choice for treatment of streptococcal APT, as there have been no reported cases of isolation of penicillin-resistant BHGAS. Amoxicillin is currently recommended for first-line treatment in some guidelines on account of its greater absorption in the gut and adequate tolerability of the oral suspension. In our survey, more than 50% of respondents prescribed amoxicillin. This could be due to several reasons: greater familiarity with the use of amoxicillin, the poor palatability and potential interference of food with drug absorption of the dosage form of penicillin V potassium (powder packets) and, possibly, providers not being aware that penicillin G benzathine is available as oral suspension, which improves palatability and does not require fasting for adequate absorption. Based on the current evidence, clavulanic acid does not offer any added benefits, as BHGAS does not produce beta-lactamases; it was only prescribed by a minority of respondents (0.6%) as amoxicillin-clavulanic acid.8-11 The prescribed regimen should be effective and facilitate adherence: oral penicillin should be prescribed at doses given every 12 hours and amoxicillin can be given at 12- or 24-hour intervals.8-11 The recommended total duration of treatment with beta-lactam antibiotics continues to be 10 days, as shorter courses have been found to achieve a lower BHGAS eradication rate8-11; however, nearly 20% of respondents reported prescribing other durations.
When it came to the items regarding the hypothetical clinical cases, the questionnaire did not provide the diagnosis because we hoped to approximate the circumstances of a real-world visit. The aspects of prescription assessed by these items are the same aspects assessed by studies of real prescription practices in patients without a microbiological diagnosis.
The first case described a patient with bronchospasm or acute bronchitis of short duration with two possible presentations: with fever and without fever. Antibiotherapy is not considered appropriate in either case. We found that 97% of respondents agreed with current recommendations in the absence of fever, but in the case of high-fever of 3 days’ duration, only 50% refrained from prescribing antibiotherapy.
The following 3 cases corresponded to 3 possible versions of common cold or upper respiratory infection: low-grade fever and clear nasal discharge, high fever and clear nasal discharge, and low-grade fever with greenish and thick nasal discharge. We considered that antibiotherapy was not indicated in any of these cases. Nearly all respondents (90.4%) agreed with this approach in the absence of high fever or green and thick mucus, but in the case of high fever, this percentage dropped to 50%, and in the case of green mucus to 59%.
Items 25 and 26 referred to a case of bronchiolitis in an infant aged 3 months, afebrile and with high fever, respectively. In the absence of fever, nearly 95% of respondents reported not prescribing antibiotics, the answer considered correct, but in the presence of high fever, despite a negative urine culture, the percentage that refrained from prescribing antibiotics decreased to 58%. In this second case of bronchiolitis, we considered either option correct (not prescribing or sometimes prescribing antibiotics), since the age of only 3 months of the hypothetical patient involved a state of physiological immunodeficiency and a deficient immunization status associated with a greater vulnerability to bacterial infection, and the clinical presentation overlapped and was indistinguishable from that of interstitial pneumonia.
Thus, in the case of infections highly likely to have a viral aetiology, such as upper respiratory tract infection, bronchospasm and bronchiolitis, we found a tendency toward the inappropriate prescription of antibiotics that was significantly associated with the presence of high fever or green nasal secretions. We ought to highlight that many viral infections manifest with high fever and that high temperatures are not necessarily associated with greater severity. Many health care users and providers believe that green and thick mucus is indicative of bacterial superinfection, when in fact it results from the release of peroxidase by leukocytes present in the secretions.
When it comes to the management of community-acquired pneumonia (CAP), many current guidelines do not recommend routine performance of chest X-rays at the primary care level and instead call for diagnosis based exclusively on clinical features.22,23 A chest radiograph would be indicated in the following cases: uncertain diagnosis, severe illness or suspected complications (such as pleural effusion), previous history of pneumonia, prolonged illness, poor response to treatment or to obtain epidemiological data. Although it may seem that not performing an X-ray could predispose to antibiotic overprescription due to inaccurate diagnosis, some studies have found the exact opposite, as visualization of atelectasis or infiltrates of viral aetiology could prompt initiation of unnecessary antibiotherapy.23 In our survey, nearly 60% of respondents reported not doing chest radiographs, which was significantly and inversely associated with the years of professional experience, as more experienced providers were less likely to order chest radiographs. For the purpose of our study, we considered any of the 3 answer choices correct (yes/no/sometimes) since some guidelines still propose the use of plain radiography to confirm the diagnosis and some respondents worked in the hospital setting (16.3%). Ninety-four percent of respondents prescribed amoxicillin for first-line treatment, consistent with current scientific evidence. The duration of treatment in typical CAP ranges from 7 to 10 days, and should be kept to 7 days in case of a good response. Shortening antibiotherapy courses in various infectious diseases, including pneumonia and AOM, is one of the strategies proposed by the World Health Organization to contain the development of antimicrobial drug resistance. Although some studies have found favourable outcomes with treatments as short as 5 days, the evidence on this aspect is still insufficient.
In the case of atypical CAP, nearly 98% of respondents correctly selected the option of treatment with macrolides such as clarithromycin or azithromycin.
Overall, the prescription by respondents of amoxicillin-clavulanic acid, cephalosporins and macrolides was infrequent for every disease, reflecting rational use of antibiotics.
According to our results, professionals are sometimes pressured by caregivers to prescribe antibiotics to children for diseases that do not require it, and they only agree to do it in some instances. This evinces a lack of awareness in the population as to the indications of antibiotic treatment in paediatric infectious diseases and a need for health education on the subject.
An essential strategy for improving antibiotic use is the education of the population through programmes focused on the use and indication of antibiotics, especially in regions where such information is most needed. In addition to the use of education campaigns, we have to take into account that the attitude of paediatric care providers over several visits can also provide perspective to the caregivers of our patients.
Antimicrobial stewardship in paediatric practice, especially at the primary care level, requires the availability of resources to diagnose illness as accurately, quickly and inexpensively as possible. Our survey shows that microbiological tests for diagnosis of pharyngitis are widely available in Spain, and that the RDT is the gold standard used at the primary care level. Introducing the use of pneumatoscopy would probably be useful to improve the assessment of otitis media, either acute or serous, as it is a technique used in conventional otoscopy that can be performed quickly and with inexpensive equipment. Another improvement measure we would recommend would be making rapid tests for detection of viral antigens (most importantly, respiratory syncytial virus and influenza) and for measurement of C-reactive protein levels in capillary blood (which would be more costly) available in primary care centres.28
When it came to the factor that respondents considered contributed most to the inappropriate use of antibiotics, more than 40% selected physician workload. In the statistical analysis, we found that physician workload was associated with not performing microbiological tests for pharyngitis, which could have increased the use of antimicrobials for management of this disease, although we did not find an association with the total score in the questionnaire, which reflected overall adherence to current clinical guidelines. Other determinants identified by the respondents were the pressure exerted by parents or caregivers, the need to be efficient in everyday practice by avoiding new visits and evaluations and the practice of defensive medicine out of fear of suits in case of poor outcomes.
There are three relatively recent publications that present data from surveys of antibiotic prescription in paediatric practice in Spain.29-31 One of them presented the results of the nationwide ABES study conducted by the Committee on Medicines of the AEP, with a large sample of more than 1200 completed questionnaires, to analyse the selection of the first-line antibiotic in most paediatric infections treated at both the ambulatory and inpatient levels.30 In this study, more experienced paediatricians obtained better scores, contrary to our study, which had a much smaller sample. This discrepancy could be explained by the more recent and updated education of younger paediatricians in our survey.
Another of the articles describes the prescription practices of paediatricians in the Valencian Community in the management of AOM and APT.31 Compared to this survey, published in 2003, we found a clear improvement in antimicrobial prescription for AOM: more than 48% of participants in the past survey reported prescribing antibiotherapy in every case, compared to 3.7% of respondents in our survey, and 63.6% prescribed amoxicillin-clavulanic acid, a very high proportion compared to the 1.1% found in our study.
Also, comparing our findings to another article published in 2005 on the use of antimicrobials for management of respiratory illness in the paediatric population of the Community of Madrid, we found an improvement in prescribing on account of the infrequent use of amoxicillin-clavulanic acid by respondents, in addition to a similar pressure by parents to prescribe antibiotherapy counter to the judgment of the clinician.29
CONCLUSION
- Antibiotherapy is prescribed when it is not necessary, especially in cases of upper respiratory infection, bronchiolitis and bronchitis associated with high fever or green nasal discharge.
- The selection of the antibiotic for first-line treatment in each of the diseases under consideration was correct and in adherence with current guidelines in a high percentage of respondents, with infrequent prescription of amoxicillin-clavulanic acid, cephalosporins and macrolides under appropriate circumstances.
- There was considerable heterogeneity in the approach to treatment of probable streptococcal pharyngitis in the absence of microbiological confirmation. Higher workloads were associated with less frequent performance of RDTs, which results in overprescription of antibiotherapy for illnesses that do not require it. A reduction in physician workloads would improve adherence to diagnostic and therapeutic clinical practice guidelines.
- More experienced physicians obtained lower scores in the questionnaire, which may suggest that as age increases, the knowledge of physicians is not as up-to-date and their practices adhere less to guidelines based on more robust evidence. Younger physicians adhered more to evidence-based practices and updated clinical practice guidelines.
- The use of chest radiographs in the case of suspected typical pneumonia in otherwise healthy children decreased with the years of experience of physicians, which entailed a decrease in the exposure to radiation and inappropriate use of antibiotics.
- Paediatricians exhibited greater knowledge of treatment protocols and answered more questions correctly compared to physicians who had not specialised in paediatrics that delivered paediatric care.
- Pathways must be set up to deliver training to professionals with the purpose of improving antibiotic prescription and health education interventions in the general population so that antibiotherapy is not demanded for illnesses for which it is not needed.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose in relation to the preparation and publication of this article.
ABBREVIATIONS
AEP: Asociación Española de Pediatría · AEPap: Asociación Española de Pediatría de Atención Primaria · AOM: acute otitis media · AP: acute pharyngotonsillitis · BHGAS: beta-haemolytic group A streptococcus · CAP: community-acquired pneumonia · CRP: C-reactive protein · RDT: rapid diagnostic test.
REFERENCES
- De la Flor i Brú J. ¿Dónde estamos 30 años después? Análisis descriptivo de un año en una consulta pública de Pediatría de Atención Primaria. Pediatr Integral. 2012; XVI:180-2.
- SEIMC, SEFH y Sociedad Española de Medicina Preventiva, Salud Pública e Higiene. Documento de consenso - Acciones y medidas para combatir las resistencias bacterianas en España, una de las mayores amenazas para la salud pública. In: Asociación Española de Pediatría [online] [accessed 03/11/2021]. Available at www.aeped.es/sites/default/files/documento_de_consenso_seimc-sefh-sempsph_sobre_resistencias_bacterianas.pdf
- ECDC country visit to Spain to discuss antimicrobial resistance issues. In: European Centre for Disease Prevention and Control [online] [accessed 03/11/2021]. Available at https://www.ecdc.europa.eu/en/publications-data/ecdc-country-visit-spain-discuss-antimicrobial-resistance-issues
- López González G, Martínez Antón A, Ruiz Contreras J. Otitis media aguda (v.2/2008). In: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [online] [accessed 03/11/2021]. Available at http://infodoctor.org/gipi/guia_abe/
- Del Castillo Martín F, Baquero Artigao F, García Migue MJ, Méndez Echevarría A. Otitis media aguda. Protoc Diagn Ter Pediatr. 2011;1:67-76.
- Del Castillo Martín F, Baquero Artigao F, de la Calle Cabrera T, López Robles MV, Ruiz Canela J, Alfayate Miguelez S, et al. Documento de consenso sobre etiología, diagnóstico y tratamiento de la otitis media aguda. An Pediatr (Barc). 2012;77:345.e1-345.e8.
- Cubero Santos A, García Vera C, Lupiani Castellanos P. Otitis media aguda. In: Guía de Algoritmos en Pediatría de Atención Primaria [online] [accessed 03/11/2021]. Available at https://algoritmos.aepap.org/algoritmo/37/otitis-media-aguda
- Fernández-Cuesta Valcarce MA, Benedicto Subirá C. Faringitis aguda (v.3/2011). In: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [online] [accessed 03/11/2021]. Available at www.guia-abe.es/temas-clinicos-faringitis-aguda
- Álvez González F, Sánchez Lastres JM. Faringoamigdalitis aguda. Protoc diagn ter pediatr. 2011;1:25-36.
- Piñeiro Pérez R, Hijano Bandera F, Álvez González F, Fernández Landaluce A, Silva Rico JC, Pérez Cánovas C, et al. Documento de consenso sobre el diagnóstico y tratamiento de la faringoamigdalitis aguda. An Pediatr (Barc). 2011;75(5):342.e1-342.e13
- Cubero Santos A, García Vera C, Lupiani Castellanos P. Faringoamigdalitis. In: Guía de Algoritmos en Pediatría de Atención Primaria [online] [accessed 03/11/2021]. Available at https://algoritmos.aepap.org/algoritmo/13/faringoamigdalitis
- Albi Rodríguez MS, Reig Rincón de Arellano I. Bronquitis (traqueobronquitis) aguda (v.2.0/2019). In: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [online] [accessed 03/11/2021]. Available at www.guia-abe.es/temas-clinicos-bronquitis-(traqueobronquitis)-aguda
- Calvo Rey C, García García ML, Casas Flecha I, Pérez Breña P. Infecciones respiratorias virales. Protoc Diagn Ter Pediatr. 2011;1:189-204.
- Castillo Laita JA, de Benito Fernández J, Escribano Montaner A, Fernández Benítez M, García de la Rubia S, Garde Garde J, et al. Consenso sobre tratamiento del asma. An Pediatr (Barc). 2007;67:253-73.
- Cortés Rico O, Rodríguez Fernández-Oliva CR. Crisis de asma. In: Guía de Algoritmos en Pediatría de Atención Primaria [online] [accessed 03/11/2021]. Available at https://algoritmos.aepap.org/algoritmo/35/crisis-de-asma
- González Requejo A. Catarro de vías altas (v.3/2015). In: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [online] [accessed 03/11/2021]. Available at www.guia-abe.es/gestion/includes/html4pdf.php?id=catarro-de-vias-altas
- Pavo García MR, Rojo Conejo P, Baro Fernández M. Bronquiolitis (v.3/2014). In: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [online] [accessed 03/11/2021]. Available at www.guia-abe.es/
- García García ML, Korta Murua J, Callejón Callejón A. Bronquiolitis aguda viral. Protoc Diagn Ter Pediatr. 2017;1:85-102.
- Cano Garcinuño A, Mora Gandarillas I, García Merino A. Bronquiolitis. In: Guía de Algoritmos en Pediatría de Atención Primaria [online] [accessed 03/11/2021]. Available at https://algoritmos.aepap.org/
- Hernández Merino A, Guerra García F. Neumonía (v.2/2008). In: Guía-ABE. Infecciones en Pediatría. Guía rápida para la selección del tratamiento antimicrobiano empírico [online] [accessed 03/11/2021]. Available at http://www.guia-abe.es
- Méndez Echevarría A, García Miguel MJ, Baquero Artigao F, Del Castillo Martín F. Neumonía adquirida en la comunidad. Protoc diagn ter pediatr. 2011;1:59-66.
- Úbeda Sansano MI, Murcia García J, Asensi Monzó MT; Grupo de Vías Respiratorias. Neumonía adquirida en la comunidad. El pediatra de Atención Primaria y la Neumonía. In: Respirar.org [online] [accessed 03/11/2021]. Available at www.respirar.org/index.php/grupo-vias-respiratorias/protocolos
- Úbeda Sansano MI, Murcia García J. Guía de Algoritmos en Pediatría de Atención Primaria. Neumonía adquirida en la comunidad. AEPap. 2017 [online] [accessed 02/01/2019]. Available at https://algoritmos.aepap.org/
- Gorrotxategi Gorrotxategi P, García Vera C, Graffigna Lojendio A, Sánchez Pina C, Palomino Urda N, Rodríguez Fernández-Oliva CR, et al. Situación de la Pediatría de Atención Primaria en España en 2018. Rev Pediatr Aten Primaria. 2018;20:e89-e104.
- Grupo de Patología Infecciosa, AEPap. Uso racional de antibióticos y Resistencias bacterianas. [online] [accessed 01/03/2020]. Available at www.aepap.org/grupos/grupo-de-patologia-infecciosa/uso-racional-de-antibioticos-y-resistencias-bacterianas
- Venekamp RP, Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2013;(1):CD000219.
- Álvez F. Uso racional de antibióticos en las infecciones más comunes de los niños. An Pediatr Contin. 2010;8:221-30.
- De la Flor i Brú J, Marés Bermúdez J. Test de diagnóstico microbiológico rápido en la consulta de Pediatría de Atención Primaria. Pediatr Integral. 2018;XXII:246.e1-246.e9.
- Herranz Jordán B, Pérez Martín C. Encuesta sobre prescripción de antibióticos en infecciones respiratorias pediátricas. Rev Pediatr Aten Primaria. 2005;7:557-78.
- Piñeiro Pérez R, Calvo Rey C, Medina Claros A.F, Bravo Acuña J, Cabrera García l, Fernández-Llamazares CM, et al. Uso empírico de antibióticos en niños en España. Resultados de una Encuesta Pediátrica Nacional 2012 (Estudio ABES). An Pediatr (Barc). 2013;79:32-41.
- Casaní Martínez C, Calvo Rigual F, Peris Vidal A, Álvarez de Lavida Mulero T, Díez Domingo J, Graullera Millas M, et al. Encuesta sobre el uso racional de antibióticos en Atención Primaria. An Pediatr. 2003;58:10-6.
Comments
This article has no comments yet.